Disease Control and Prevention Center, National Center for Global Health and Medicine, 1-21-1 Toyama, Shinjuku-ku, Tokyo, 162-8655, Japan; Emerging and Reemerging Infectious Diseases, National Center for Global Health and Medicine, Graduate School of Medicine, Tohoku University, 2-1 Seiryo-cho, Aoba-ku, Sendai City, Miyagi 980-8575, Japan.
Disease Control and Prevention Center, National Center for Global Health and Medicine, 1-21-1 Toyama, Shinjuku-ku, Tokyo, 162-8655, Japan.
J Infect Chemother. 2021 Nov;27(11):1669-1673. doi: 10.1016/j.jiac.2021.08.015. Epub 2021 Aug 14.
The automated quantitative antigen test (QAT), which detects severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), is suitable for mass screening. However, its diagnostic capability differentiated by time from onset and potential contribution to infectivity assessment have not been fully investigated.
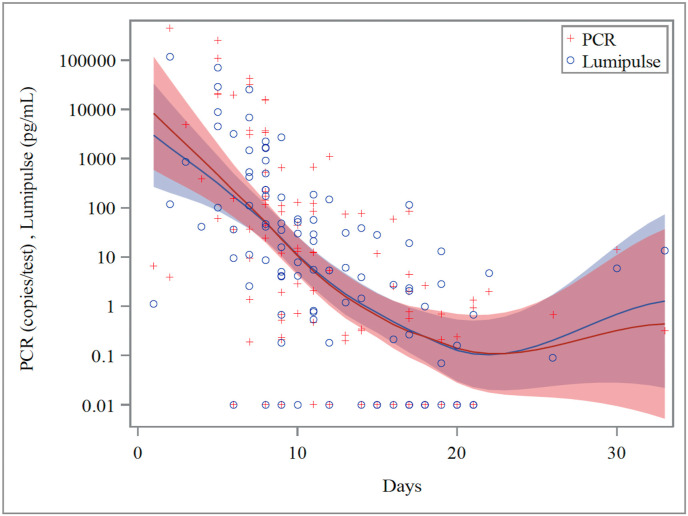
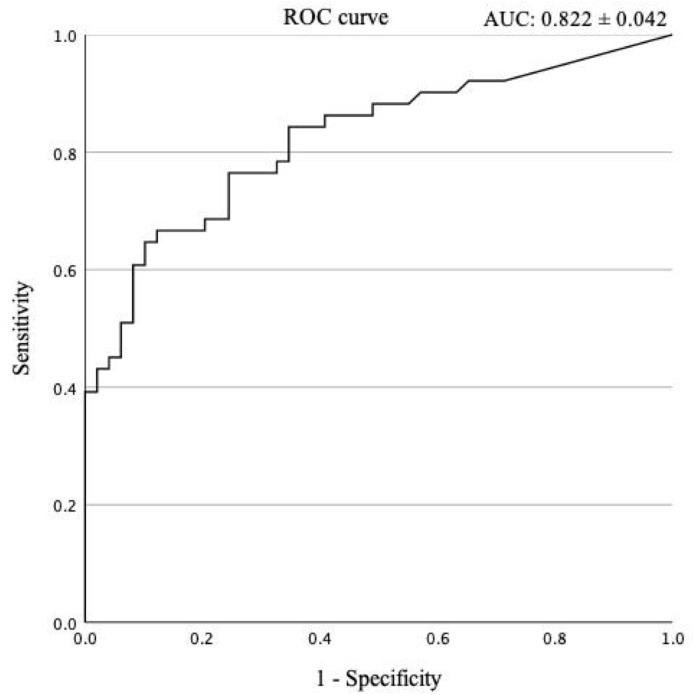
A retrospective, observational study using nasopharyngeal swab specimens from coronavirus disease (COVID-19) inpatients was conducted using Lumipulse SARS-CoV-2 antigen test. Diagnostic accuracy was examined for the early (up to 10 days after onset) and late (over 10 days after onset) stages. Time-course QAT changes and reverse-transcription quantitative polymerase chain reaction tests results were displayed as locally estimated scatterplot smoothing curve, and receiver operating characteristic curve (ROC) analysis was used to determine the appropriate cutoff value for differentiating the early and late stages.
We obtained 100 specimens from 68 COVID-19 patients, including 51 early-stage and 49 late-stage specimens. QAT sensitivity and specificity were 0.82 (0.72-0.90) and 0.95 (0.75-0.99) for all periods, 0.93 (0.82-0.98) and 1.00 (0.39-1.00) for the early stage, and 0.66 (0.48-0.82) and 0.93 (0.69-0.99) for the late stage, respectively. The ROC analysis indicated an ideal cutoff value of 6.93 pg/mL for distinguishing early-from late-stage specimens. The sensitivity, specificity, positive predictive value, and negative predictive value for predicting the late stage were 0.76 (0.61-0.87), 0.76 (0.63-0.87), 0.76 (0.61-0.87), and 0.76 (0.63-0.87).
QAT has favorable diagnostic accuracy in the early COVID-19 stages. In addition, an appropriate cutoff point can potentially facilitate rapid identification of noncontagious patients.
用于检测严重急性呼吸综合征冠状病毒 2(SARS-CoV-2)的自动化定量抗原检测(QAT)适用于大规模筛查。然而,其在发病时间上的诊断能力以及对传染性评估的潜在贡献尚未得到充分研究。
使用 Lumipulse SARS-CoV-2 抗原检测对来自冠状病毒病(COVID-19)住院患者的鼻咽拭子标本进行回顾性、观察性研究。检测了早期(发病后 10 天内)和晚期(发病后 10 天以上)的诊断准确性。QAT 变化的时间过程和逆转录定量聚合酶链反应检测结果显示为局部估计散点平滑曲线,并使用接收者操作特征曲线(ROC)分析来确定区分早期和晚期的适当截断值。
我们从 68 例 COVID-19 患者中获得了 100 份标本,其中 51 份为早期标本,49 份为晚期标本。QAT 的敏感性和特异性在所有时间段均为 0.82(0.72-0.90)和 0.95(0.75-0.99),早期阶段为 0.93(0.82-0.98)和 1.00(0.39-1.00),晚期阶段为 0.66(0.48-0.82)和 0.93(0.69-0.99)。ROC 分析表明,区分早期和晚期标本的理想截断值为 6.93 pg/mL。预测晚期的敏感性、特异性、阳性预测值和阴性预测值分别为 0.76(0.61-0.87)、0.76(0.63-0.87)、0.76(0.61-0.87)和 0.76(0.63-0.87)。
QAT 在 COVID-19 的早期阶段具有良好的诊断准确性。此外,适当的截断值可能有助于快速识别非传染性患者。