Doroshow Deborah B, Wei Wei, Gupta Swati, Zugazagoitia Jon, Robbins Charles, Adamson Blythe, Rimm David L
Division of Hematology and Medical Oncology, Tisch Cancer Institute, Icahn School of Medicine at Mount Sinai, New York, New York.
Department of Biostatistics, Yale School of Public Health, New Haven, Connecticut.
J Thorac Oncol. 2021 Dec;16(12):2139-2143. doi: 10.1016/j.jtho.2021.07.032. Epub 2021 Aug 26.
For patients with NSCLC receiving immune checkpoint inhibitors, programmed death-ligand 1 (PD-L1) tumor proportion score (TPS) has been validated as a predictive biomarker for improved overall survival (OS). Nevertheless, its histology-specific predictive value in patients with advanced squamous versus nonsquamous cancers remains unclear. To evaluate the differential value of PD-L1 TPS as a predictive biomarker for OS after first-line pembrolizumab in patients with squamous versus nonsquamous NSCLC.
Retrospective, observational study of patients diagnosed with having advanced NSCLC who were treated between October 2015 and April 2019 at community oncology clinics and academic medical centers in a deidentified electronic health record-derived database. Included patients were diagnosed with having advanced or metastatic NSCLC, received treatment with first-line, single-agent pembrolizumab, and had documentation of PD-L1 testing with a numeric result. Exclusion criteria included alterations in EGFR, ALK, and ROS1. The primary end point was OS from start of first-line pembrolizumab therapy by squamous or nonsquamous histology and PD-1 expression level measured by TPS (low, <50% or high, ≥50%).
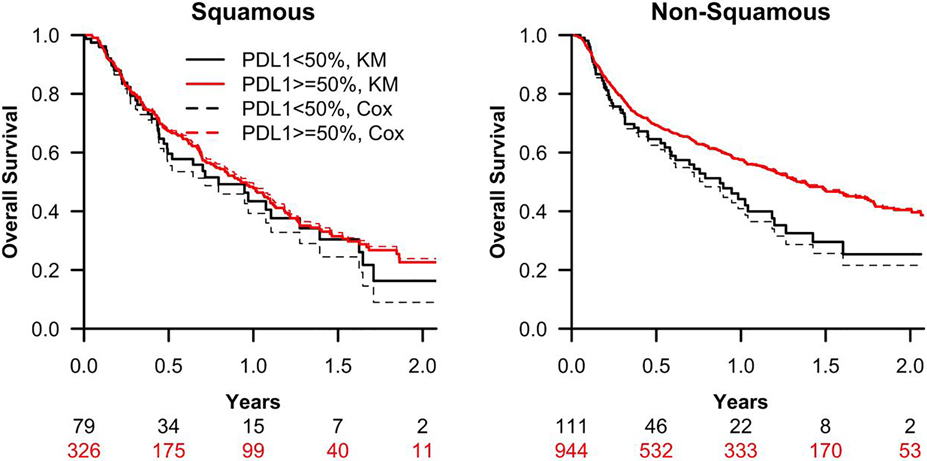
The cohort of 1460 patients with NSCLC who received pembrolizumab as a first-line therapy had a mean age of 72 years. Histology was 28% squamous and 72% nonsquamous. PD-L1 expression was low in 13% and high in 87%. No meaningful differences in age, sex, or smoking history were observed by PD-L1 TPS or histology type. A generalized gamma model adjusting for sex and stage at diagnosis found that for patients with nonsquamous histology, high PD-L1 TPS was significantly associated with improved OS by a median OS difference of 8.4 months (p < 0.001). In contrast, for patients with squamous histology, there was no evidence of association between PD-L1 expression level and OS (p = 0.283). PD-L1-related incremental differences in median OS between the patients with squamous and nonsquamous tumors were significantly different (p = 0.034).
Among patients with NSCLC treated with first-line pembrolizumab, high PD-L1 TPS is associated with OS among patients with nonsquamous NSCLC, but not among patients with squamous NSCLC.
对于接受免疫检查点抑制剂治疗的非小细胞肺癌(NSCLC)患者,程序性死亡配体1(PD-L1)肿瘤比例评分(TPS)已被确认为可改善总生存期(OS)的预测生物标志物。然而,其在晚期鳞状细胞癌与非鳞状细胞癌患者中的组织学特异性预测价值仍不明确。本研究旨在评估PD-L1 TPS作为一线帕博利珠单抗治疗后鳞状与非鳞状NSCLC患者OS预测生物标志物的差异价值。
在一个经过去识别化处理的电子健康记录衍生数据库中,对2015年10月至2019年4月期间在社区肿瘤诊所和学术医疗中心接受治疗、被诊断为晚期NSCLC的患者进行回顾性观察研究。纳入患者被诊断为晚期或转移性NSCLC,接受一线单药帕博利珠单抗治疗,且有PD-L1检测的数值结果记录。排除标准包括表皮生长因子受体(EGFR)、间变性淋巴瘤激酶(ALK)和ROS1的改变。主要终点是从一线帕博利珠单抗治疗开始按鳞状或非鳞状组织学以及通过TPS测量的PD-L1表达水平(低,<50%或高,≥50%)计算的OS。
1460例接受帕博利珠单抗一线治疗的NSCLC患者队列的平均年龄为72岁。组织学类型为28%鳞状和72%非鳞状。PD-L1表达低的占13%,高的占87%。按PD-L1 TPS或组织学类型观察,年龄、性别或吸烟史无显著差异。一个针对性别和诊断时分期进行调整的广义伽马模型发现,对于非鳞状组织学患者,高PD-L1 TPS与OS改善显著相关,中位OS差异为8.4个月(p < 0.001)。相比之下,对于鳞状组织学患者,没有证据表明PD-L1表达水平与OS之间存在关联(p = 0.283)。鳞状和非鳞状肿瘤患者之间PD-L1相关的中位OS增量差异显著不同(p = 0.034)。
在接受一线帕博利珠单抗治疗的NSCLC患者中,高PD-L1 TPS与非鳞状NSCLC患者的OS相关,但与鳞状NSCLC患者的OS无关。