Pediatric and Congenital Cardiac Surgery Unit, Department of Cardiac, Thoracic, Vascular Sciences and Public Health, University of Padova Medical School, Padova, Italy.
Unit of Biostatistics, Department of Cardiac, Thoracic, Vascular Sciences and Public Health, University of Padova Medical School, Padova, Italy.
Artif Organs. 2021 Dec;45(12):1543-1553. doi: 10.1111/aor.14057. Epub 2021 Sep 12.
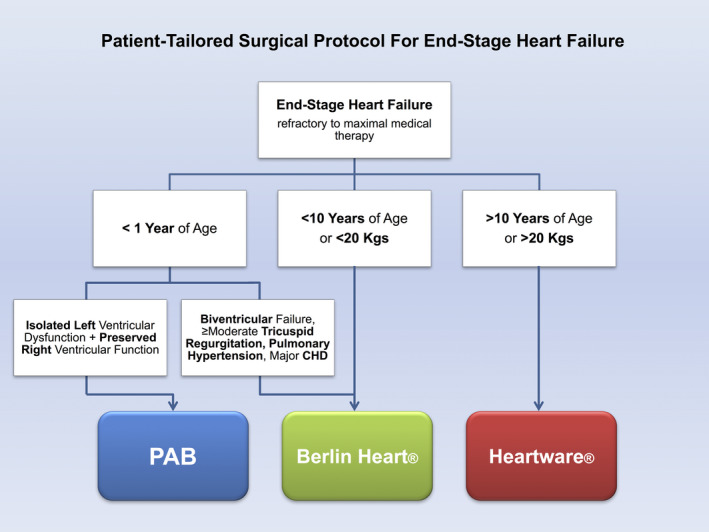
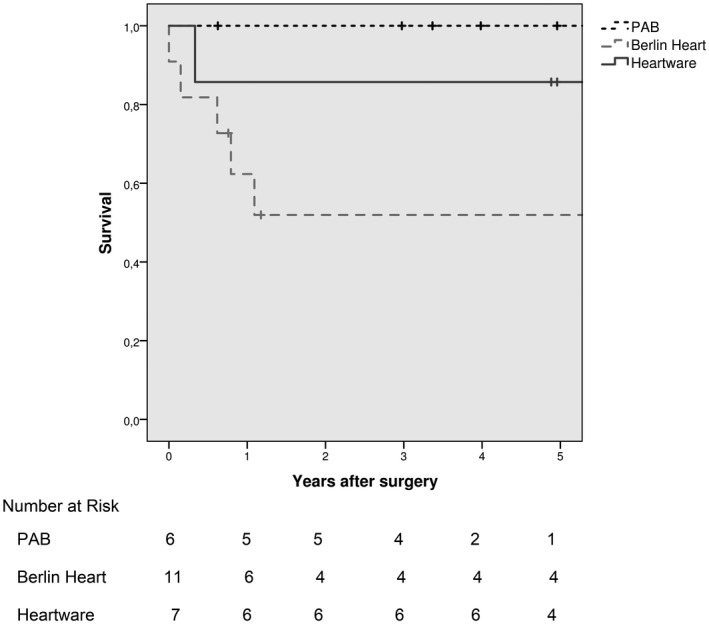
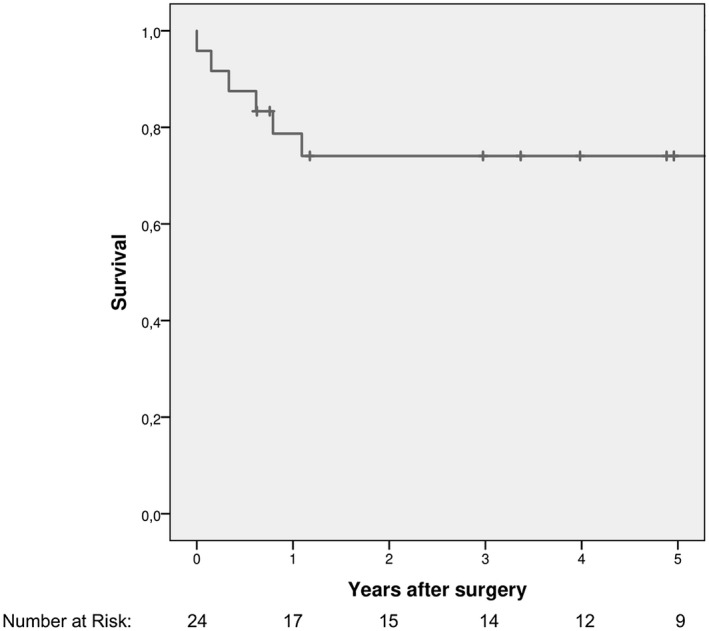
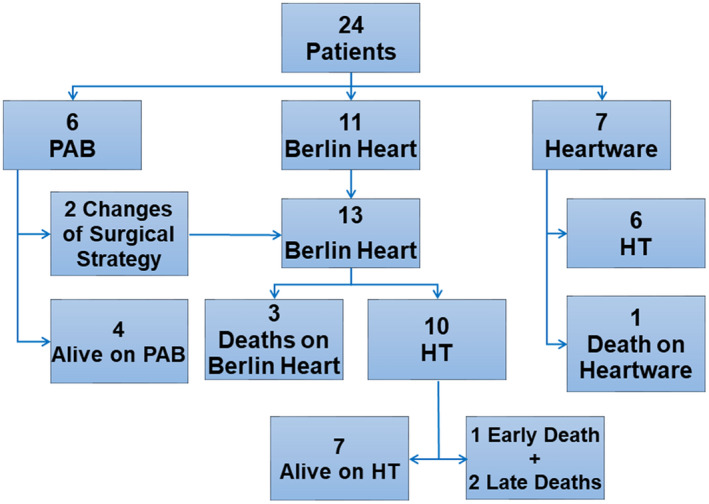
End-stage heart failure (ESHF) in pediatric age is an ongoing challenge. Heart transplantation is the final option, but its long-term outcomes are still suboptimal in children. An alternative patient-tailored surgical protocol to manage ESHF in children is described. Retrospective, single-center analysis of pediatric patients admitted to our institution between April 2004 and February 2021 for ESHF. Our current protocol is as follows: (a) Patients <1 year with isolated left ventricular dysfunction due to dilated cardiomyopathy underwent pulmonary artery banding (PAB). (b) Patients <10 years and <20 kg, who did not meet previous criteria were managed with Berlin Heart EXCOR. (c) Patients >10 years or >20 kg, underwent placement of intracorporeal Heartware. Primary outcomes were survival, transplant incidence, and postoperative adverse events. A total of 24 patients (mean age 5.3 ± 5.9 years) underwent 26 procedures: PAB in 6 patients, Berlin Heart in 11, and Heartware in 7. Two patients shifted from PAB to Berlin Heart. Overall survival at 1-year follow-up and 5-year follow-up was 78.7% (95%CI = 62%-95.4%) and 74.1% (95%CI = 56.1%-92.1%), respectively. Berlin Heart was adopted in higher-risk settings showing inferior outcomes, whereas a PAB enabled 67% of patients to avoid transplantation, with no mortality. An integrated, patient-tailored surgical strategy, comprehensive of PAB and different types of ventricular assist devices, can provide satisfactory medium-term results for bridging to transplant or recovery. The early postoperative period is critical and requires strict clinical vigilance. Selected infants can benefit from PAB that has demonstrated to be a safe bridge to recovery.
儿童晚期心力衰竭(ESHF)是一个持续存在的挑战。心脏移植是最后的选择,但在儿童中其长期结果仍不理想。描述了一种针对儿童 ESHF 的患者定制的替代手术方案。回顾性分析 2004 年 4 月至 2021 年 2 月期间因 ESHF 入住我院的儿科患者的单中心资料。我们目前的方案如下:(a)因扩张型心肌病导致孤立性左心室功能障碍的<1 岁患者行肺动脉带缩术(PAB)。(b)<10 岁且<20kg 且不符合上述标准的患者采用柏林心脏 EXCOR 治疗。(c)>10 岁或>20kg 的患者行内置 Heartware 治疗。主要结局为生存率、移植发生率和术后不良事件。共 24 例患者(平均年龄 5.3±5.9 岁)行 26 例手术:PAB 治疗 6 例,柏林心脏 11 例,Heartware 7 例。2 例患者从 PAB 转为柏林心脏。1 年和 5 年随访时的总体生存率分别为 78.7%(95%CI=62%-95.4%)和 74.1%(95%CI=56.1%-92.1%)。柏林心脏适用于风险较高的患者,其结果较差,而 PAB 可使 67%的患者避免移植,且无死亡。综合的、以患者为中心的手术策略,包括 PAB 和不同类型的心室辅助装置,可以为过渡到移植或恢复提供满意的中期结果。围手术期早期是关键,需要严格的临床监测。部分婴儿可从 PAB 中获益,PAB 已被证明是安全的恢复桥梁。