Kelly Liam P, Basset Fabien Andre, McCarthy Jason, Ploughman Michelle
Recovery and Performance Laboratory, Faculty of Medicine, Memorial University of Newfoundland, St. John's, NL, Canada.
School of Human Kinetics and Recreation, Memorial University of Newfoundland, St. John's, NL, Canada.
Front Physiol. 2021 Aug 16;12:702439. doi: 10.3389/fphys.2021.702439. eCollection 2021.
To evaluate the safety and feasibility of performing treadmill aerobic exercise in moderate normobaric hypoxia among chronic hemiparetic stroke survivors.
Observational study using convenience sampling.
Research laboratory in a tertiary rehabilitation hospital.
Chronic hemiparetic stroke survivors who could walk at least 10-m with or without assistance and had no absolute contraindications to exercise testing.
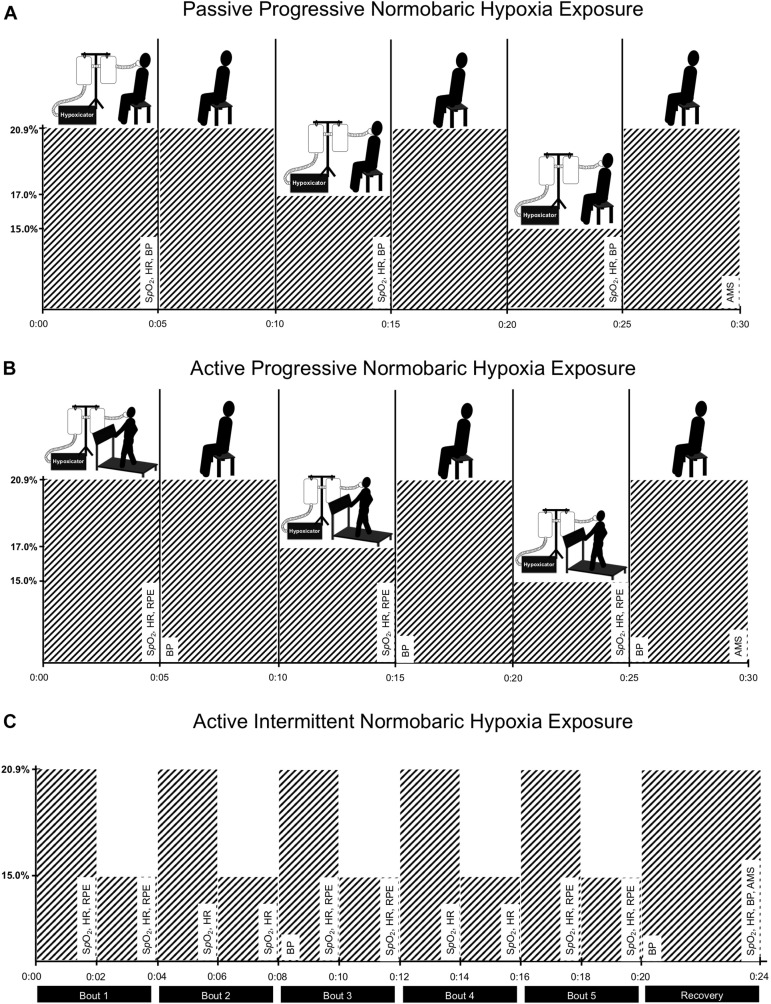
Participants (three male and four female) were asked to complete three normobaric hypoxia exposure protocols within a single session. First, they were passively exposed to normobaric hypoxia through gradual reductions in the fraction of inspired oxygen (FO = 20.9, 17.0, and 15.0%) while seated (5-min at each level of FO). Participants were then exposed to the same reductions in FO during constant-load exercise performed on a treadmill at 40% of heart rate reserve. Finally, participants completed 20-min of exercise while intermittently exposed to moderate normobaric hypoxia (5 × 2-min at FO = 15.0%) interspaced with 2-min normoxia intervals (FO = 20.9%).
The primary outcome was occurrence of adverse events, which included standardized criteria for terminating exercise testing, blood oxygen saturation (SO) <80%, or acute mountain sickness score >2. The increased cardiovascular strain imposed by normobaric hypoxia exposure at rest and during exercise was evaluated by changes in SO, heart rate (HR), blood pressure, and rating of perceived exertion (RPE).
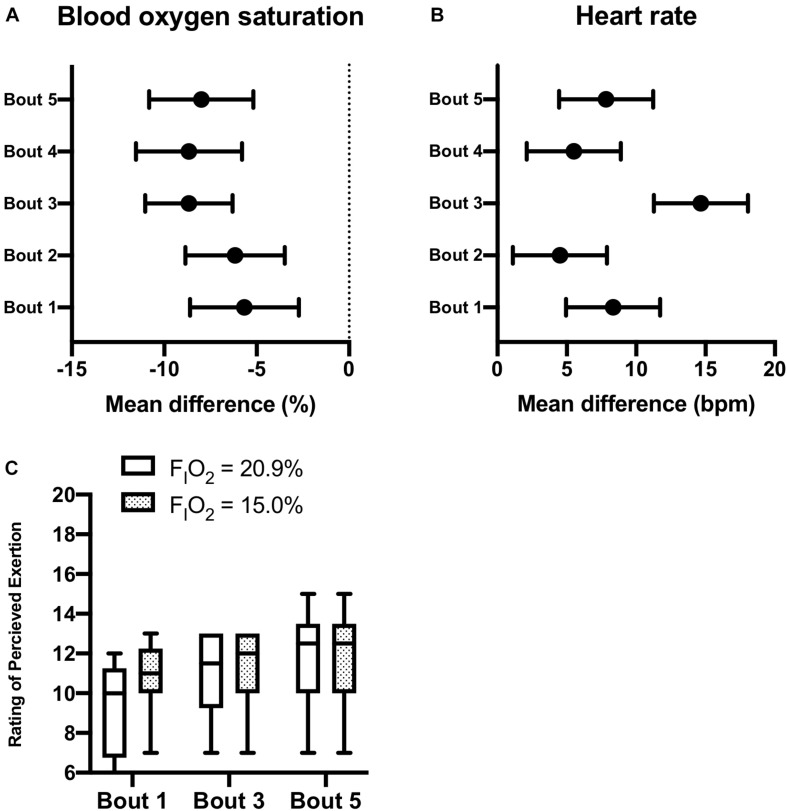
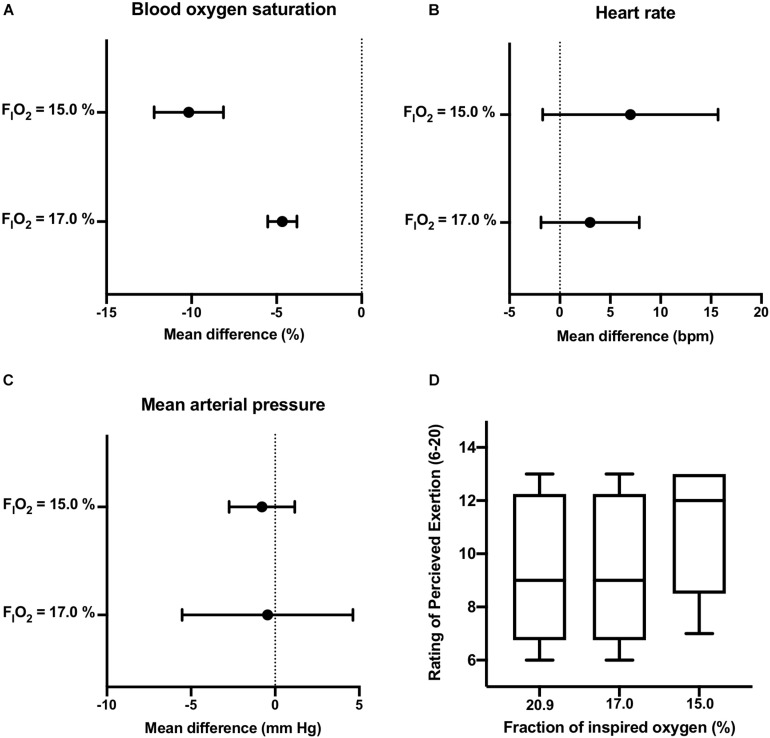
One participant reported mild symptoms of nausea during exercise in normobaric hypoxia and discontinued participation. No other adverse events were recorded. Intermittent normobaric hypoxia exposure was associated with reduced SO (MD = -7.4%, CI: -9.8 to -5.0) and increased HR (MD = 8.2, CI: 4.6 to 11.7) compared to intervals while breathing typical room air throughout the 20-min constant-load exercise period. The increase in HR was associated with a 10% increase in relative effort. However, reducing FO had little effect on blood pressure and RPE measurements.
Moderate normobaric hypoxia appeared to be a safe and feasible method to increase the cardiovascular strain of submaximal exercise in chronic hemiparetic stroke survivors. Future studies evaluating the effects of pairing normobaric hypoxia exposure with existing therapies on secondary prevention and functional recovery are warranted.
评估慢性偏瘫性卒中幸存者在中度常压缺氧环境下进行跑步机有氧运动的安全性和可行性。
采用便利抽样的观察性研究。
三级康复医院的研究实验室。
能够在有或无辅助的情况下行走至少10米且无运动测试绝对禁忌证的慢性偏瘫性卒中幸存者。
参与者(3名男性和4名女性)被要求在单个疗程内完成三个常压缺氧暴露方案。首先,他们坐在座位上,通过逐渐降低吸入氧分数(FO = 20.9%、17.0%和15.0%)被动暴露于常压缺氧环境(每个FO水平持续5分钟)。然后,参与者在跑步机上以心率储备的40%进行恒负荷运动时,暴露于相同的FO降低水平。最后,参与者在间歇性暴露于中度常压缺氧(5次,每次2分钟,FO = 15.0%)并间隔2分钟常氧期(FO = 20.9%)的情况下完成20分钟的运动。
主要观察指标为不良事件的发生情况,包括终止运动测试的标准化标准、血氧饱和度(SO)<80%或急性高山病评分>2。通过SO、心率(HR)、血压和主观用力程度分级(RPE)的变化评估在休息和运动期间常压缺氧暴露所增加的心血管负荷。
一名参与者在常压缺氧运动期间报告有轻度恶心症状并退出研究。未记录到其他不良事件。与在整个20分钟恒负荷运动期间呼吸普通室内空气的时间段相比,间歇性常压缺氧暴露与SO降低(MD = -7.4%,CI:-9.8至-5.0)和HR增加(MD = 8.2,CI:4.6至11.7)相关。HR的增加与相对用力增加10%相关。然而,降低FO对血压和RPE测量影响不大。
中度常压缺氧似乎是增加慢性偏瘫性卒中幸存者次最大运动心血管负荷的一种安全可行的方法。有必要开展进一步研究,评估将常压缺氧暴露与现有疗法相结合对二级预防和功能恢复的影响。