Rehabilitation Medicine, Amsterdam UMC, University of Amsterdam, Amsterdam Movement Sciences, Amsterdam, The Netherlands
Rehabilitation Medicine, Amsterdam UMC, University of Amsterdam, Amsterdam Movement Sciences, Amsterdam, The Netherlands.
BMJ Open Diabetes Res Care. 2021 Sep;9(1). doi: 10.1136/bmjdrc-2021-002392.
The skin of people with diabetic foot disease is thought to heat up from ambulatory activity before it breaks down into ulceration. This allows for early recognition of imminent ulcers. We assessed whether at-home monitoring of plantar foot skin temperature can help prevent ulcer recurrence in diabetes.
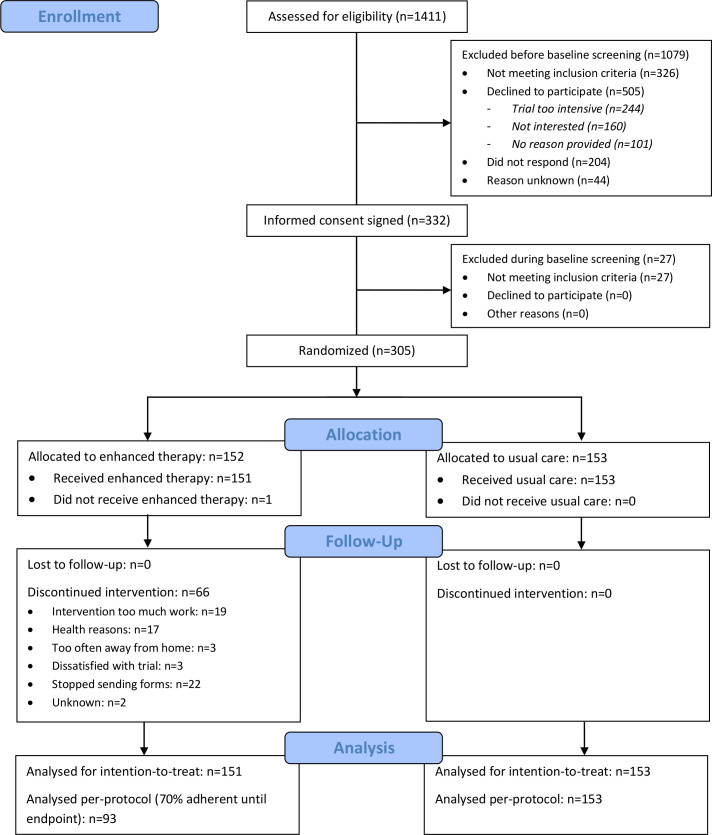
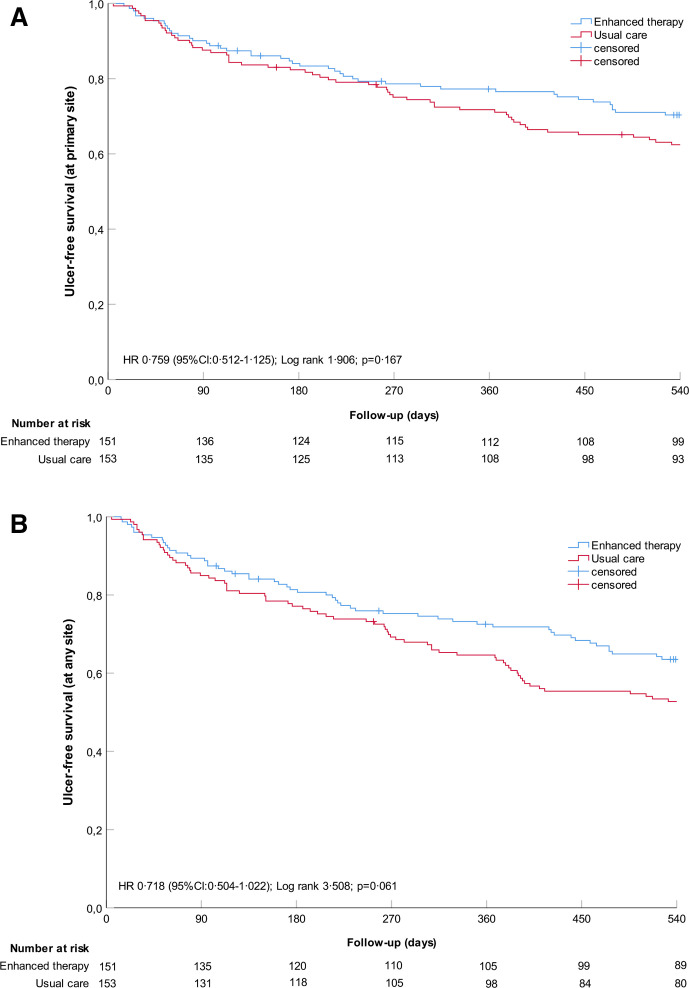
In this parallel-group outcome-assessor-blinded multicenter randomized controlled trial (7 hospitals, 4 podiatry practices), we randomly assigned people with diabetes, neuropathy, foot ulcer history (<4 years, n=295), or Charcot's neuro-arthropathy (n=9) to usual care (ie, podiatric treatment, education, and therapeutic footwear) or usual care plus measuring skin temperatures at 6-8 plantar sites per foot each day (enhanced therapy). If ∆T>2.2°C between corresponding sites on the left and right foot for two consecutive days, participants were instructed to reduce ambulatory activity until this hotspot disappeared and contact their podiatrist. Primary outcome was ulcer recurrence in 18 months on the plantar foot, interdigital, or medial/lateral/anterior forefoot surfaces; secondary outcome was ulcer recurrence at any foot site.
On the basis of intention-to-treat, 44 of 151 (29.1%) participants in enhanced therapy and 57 of 153 (37.3%) in usual care had ulcer recurrence at a primary outcome site (RR: 0.782 (95%CI 0.566 to 1.080), p=0.133). Of the 83 participants in enhanced therapy who measured a hotspot, the 24 subsequently reducing their ambulatory activity had significantly fewer ulcer recurrences (n=3) than those in usual care (RR: 0.336 (95% CI 0.114 to 0.986), p=0.017). Enhanced therapy was effective over usual care for ulcer recurrence at any foot site (RR: 0.760 (95% CI 0.579 to 0.997), p=0.046).
At-home foot temperature monitoring does not significantly reduce incidence of diabetic foot ulcer recurrence at or adjacent to measurement sites over usual care, unless participants reduce ambulatory activity when hotspots are found, or when aiming to prevent ulcers at any foot site.
NTR5403.
据认为,患有糖尿病足病的人的皮肤在出现溃疡之前会因活动而升温。这可以早期识别即将发生的溃疡。我们评估了在家中监测足底皮肤温度是否有助于预防糖尿病患者溃疡复发。
在这项平行组结局评估者盲法多中心随机对照试验(7 家医院,4 家足病诊所)中,我们将患有糖尿病、周围神经病变、足部溃疡病史(<4 年,n=295)或夏科氏神经关节病(n=9)的患者随机分为常规治疗组(即足病治疗、教育和治疗性鞋类)或常规治疗加每天测量每只脚 6-8 个足底部位的皮肤温度(增强治疗)。如果左右脚相应部位的 ∆T>2.2°C 连续两天,参与者将被指示减少活动量,直到热点消失并联系他们的足病医生。主要结局是 18 个月时足底、趾间、内侧/前足表面的溃疡复发;次要结局是任何足部部位的溃疡复发。
基于意向治疗,增强治疗组的 151 名参与者中有 44 名(29.1%)和常规治疗组的 153 名参与者中有 57 名(37.3%)在主要结局部位出现溃疡复发(RR:0.782(95%CI 0.566 至 1.080),p=0.133)。在接受增强治疗的 83 名参与者中,有 83 名测量到热点的参与者中,有 24 名随后减少了活动量,溃疡复发的人数明显少于常规治疗组(RR:0.336(95%CI 0.114 至 0.986),p=0.017)。与常规治疗相比,增强治疗对任何足部部位的溃疡复发均有效(RR:0.760(95%CI 0.579 至 0.997),p=0.046)。
在家中监测足部温度并不能显著降低与测量部位相邻或相邻的糖尿病足溃疡复发的发生率,除非参与者在发现热点时减少活动量,或者当旨在预防任何足部部位的溃疡时。
NTR5403。