Department of Cardiology, Oslo University Hospital, Rikshospitalet, Oslo, 0027, Norway.
Department of Pediatric Cardiology, Oslo University Hospital, Oslo, 0027, Norway.
ESC Heart Fail. 2021 Dec;8(6):5222-5236. doi: 10.1002/ehf2.13601. Epub 2021 Sep 12.
We tested the hypothesis that shortening of time-to-peak left ventricular pressure rise (Td) reflect resynchronization in an animal model and that Td measured in patients will be helpful to identify long-term volumetric responders [end-systolic volume (ESV) decrease >15%] in cardiac resynchronization therapy (CRT).
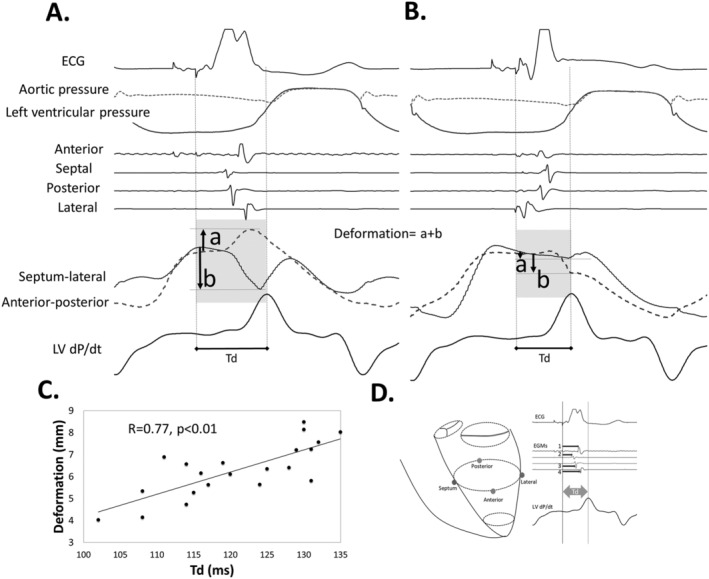
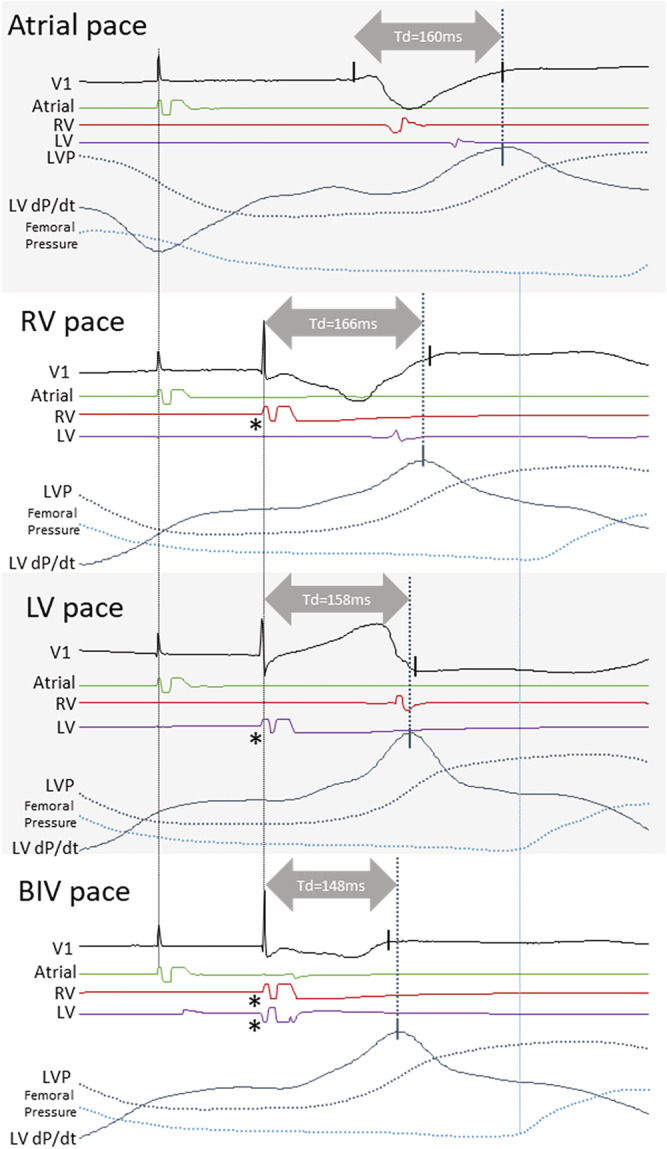
Td was analysed in an animal study (n = 12) of left bundle-branch block (LBBB) with extensive instrumentation to detect left ventricular myocardial deformation, electrical activation, and pressures during pacing. The sum of electrical delays from the onset of pacing to four intracardiac electrodes formed a synchronicity index (SI). Pacing was performed at baseline, with LBBB, right and left ventricular pacing and finally with biventricular pacing (BIVP). We then studied Td at baseline and with BIVP in a clinical observational study in 45 patients during the implantation of CRT and followed up for up to 88 months.
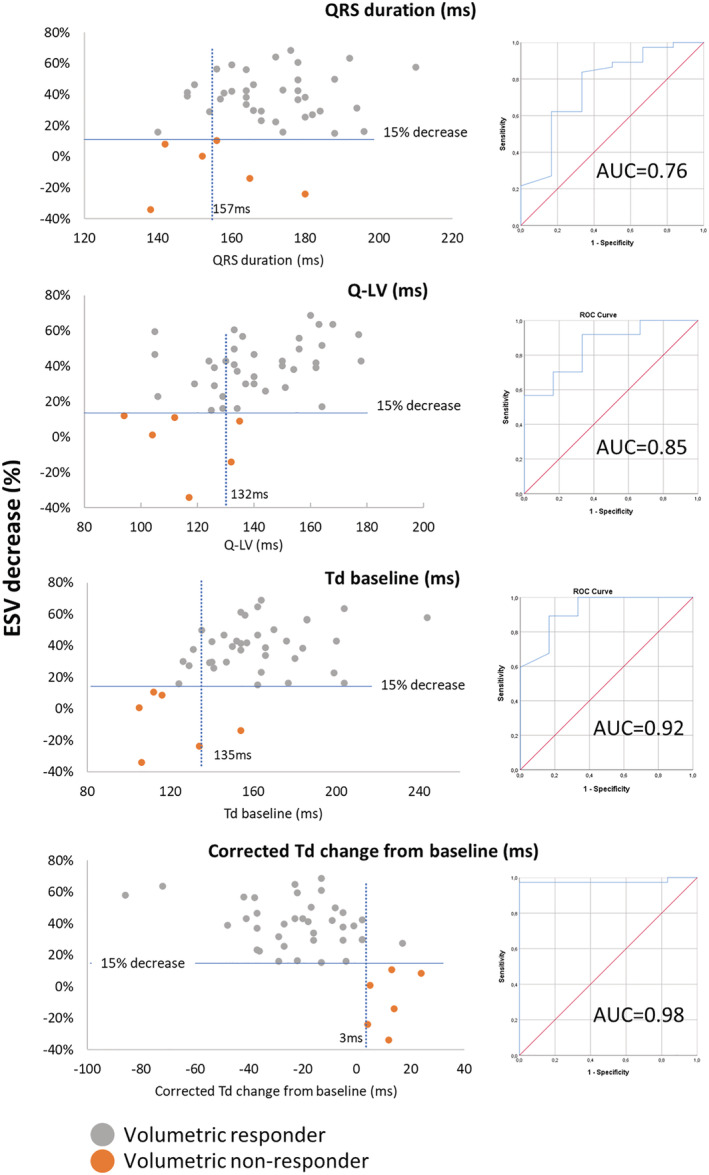
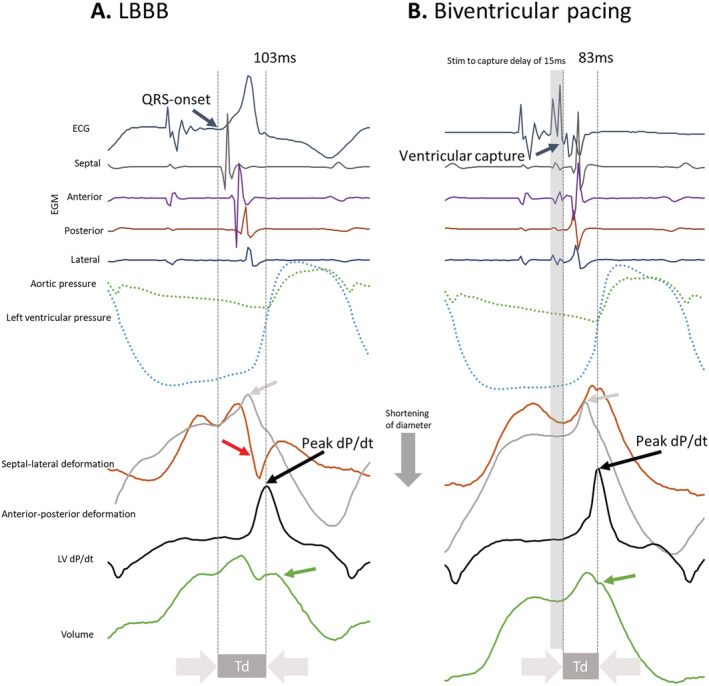
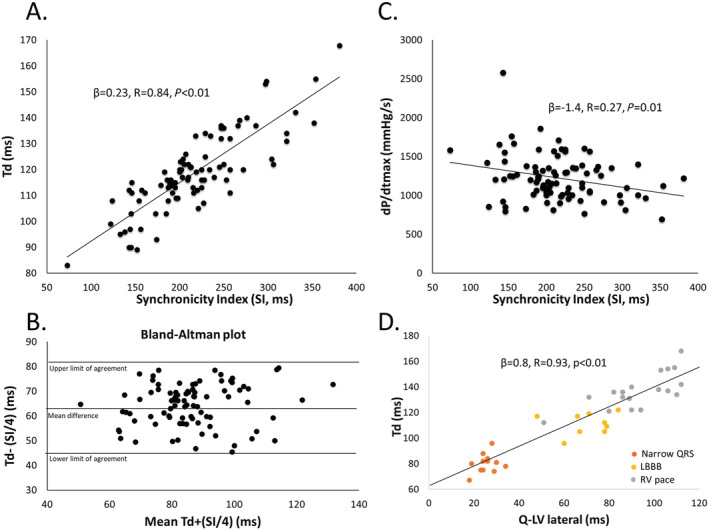
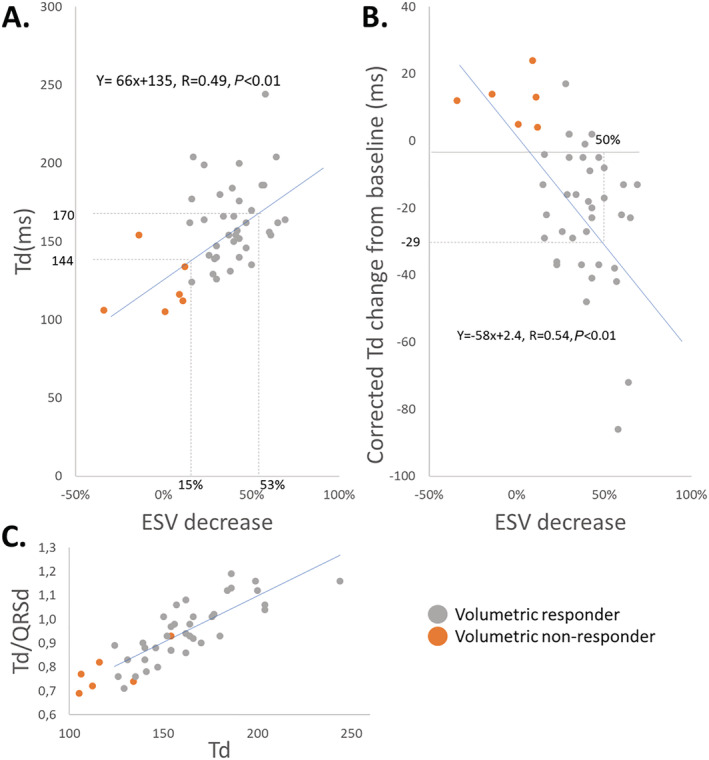
We found a strong relationship between Td and SI in the animals (R = 0.84, P < 0.01). Td and SI increased from narrow QRS at baseline (Td = 95 ± 2 ms, SI = 141 ± 8 ms) to LBBB (Td = 125 ± 2 ms, SI = 247 ± 9 ms, P < 0.01), and shortened with biventricular pacing (BIVP) (Td = 113 ± 2 ms and SI = 192 ± 7 ms, P < 0.01). Prolongation of Td was associated with more wasted deformation during the preejection period (R = 0.77, P < 0.01). Six patients increased ESV by 2.5 ± 18%, while 37 responders (85%) had a mean ESV decrease of 40 ± 15% after more than 6 months of follow-up. Responders presented with a higher Td at baseline than non-responders (163 ± 26 ms vs. 121 ± 19 ms, P < 0.01). Td decreased to 156 ± 16 ms (P = 0.02) with CRT in responders, while in non-responders, Td increased to 148 ± 21 ms (P < 0.01). A decrease in Td with BIVP to values similar or below what was found at baseline accurately identified responders to therapy (AUC 0.98, P < 0.01). Td at baseline and change in Td from baseline was linear related to the decrease in ESV at follow-up. All-cause mortality was high among six non-responders (n = 4), while no patients died in the responder group during follow-up.
Prolongation of Td is associated with cardiac dyssynchrony and more wasted deformation during the preejection period. Shortening of a prolonged Td with CRT in patients accurately identifies volumetric responders to CRT with incremental value on top of current guidelines and practices. Thus, Td carries the potential to become a biomarker to predict long-term volumetric response in CRT candidates.
我们检验了以下假说,即左心室压力上升时间峰值(Td)缩短反映了动物模型中的再同步,并且患者的 Td 测量将有助于识别心脏再同步治疗(CRT)的长期容量反应者[收缩末期容积(ESV)下降> 15%]。
在左束支传导阻滞(LBBB)的动物研究(n = 12)中分析了 Td,该研究广泛使用了仪器来检测左心室心肌变形、电激活和起搏期间的压力。从起搏开始到四个心内电极的电延迟总和形成同步指数(SI)。起搏在基线、LBBB、右心室和左心室起搏以及最后进行双心室起搏(BIVP)时进行。然后,我们在 CRT 植入期间对 45 例患者的临床观察研究中研究了基线和 BIVP 时的 Td,并进行了长达 88 个月的随访。
我们发现动物体内 Td 和 SI 之间存在很强的关系(R = 0.84,P < 0.01)。Td 和 SI 从基线时的窄 QRS 增加(Td = 95 ± 2 ms,SI = 141 ± 8 ms)到 LBBB(Td = 125 ± 2 ms,SI = 247 ± 9 ms,P < 0.01),并随双心室起搏(BIVP)而缩短(Td = 113 ± 2 ms,SI = 192 ± 7 ms,P < 0.01)。Td 的延长与射前期更多的浪费变形有关(R = 0.77,P < 0.01)。6 例患者的 ESV 增加了 2.5 ± 18%,而 37 例反应者(85%)在超过 6 个月的随访后,ESV 平均下降了 40 ± 15%。与非反应者相比,反应者的 Td 在基线时更高(163 ± 26 ms 与 121 ± 19 ms,P < 0.01)。在反应者中,随着 CRT 的应用,Td 降低至 156 ± 16 ms(P = 0.02),而在非反应者中,Td 增加至 148 ± 21 ms(P < 0.01)。BIVP 后 Td 降低至与基线相似或低于基线的水平,可准确识别治疗反应者(AUC 0.98,P < 0.01)。基线 Td 和基线 Td 的变化与随访时 ESV 的下降呈线性相关。在六个非反应者中(n = 4),有六名患者死亡,而在反应者组中,在随访期间没有患者死亡。
Td 的延长与射前期的心脏不同步和更多的浪费变形有关。在患者中,随着 CRT 的应用,延长的 Td 缩短,可以准确识别 CRT 的容量反应者,在现有指南和实践的基础上增加了额外的价值。因此,Td 有可能成为预测 CRT 候选者长期容量反应的生物标志物。