Department of Radiology, West China Hospital, Sichuan University, Chengdu, Sichuan, China.
Department of Radiology, Sichuan Cancer Hospital and Institute, Sichuan Cancer Center, School of Medicine, University of Electronic Science and Technology of China, Chengdu, Sichuan, China.
Cardiovasc Diabetol. 2021 Sep 14;20(1):185. doi: 10.1186/s12933-021-01379-3.
Heart failure with preserved ejection fraction (HFpEF) is a heterogeneous syndrome with sex-specific pathophysiology. Estrogen deficiency is believed to be responsible for the development of HFpEF in women. However, estrogen deficiency does not seem to be completely responsible for the differences in HFpEF prevalence between sexes. While diabetes mellitus (DM) frequently coexists with HFpEF in women and is associated with worse outcomes, the changes in myocardial contractility among women with HFpEF and the DM phenotype is yet unknown. Therefore, we aimed to investigate sex-related differences in left ventricular (LV) contractility dysfunction in HFpEF comorbid with DM.
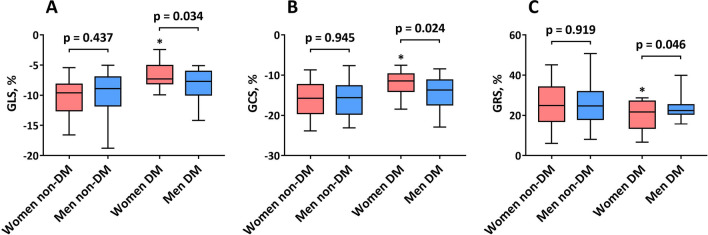
A total of 224 patients who underwent cardiac cine MRI were included in this study. Sex-specific differences in LV structure and function in the context of DM were determined. LV systolic strains (global longitudinal strain [GLS], circumferential strain [GCS] and radial strain [GRS]) were measured using cine MRI. The determinants of impaired myocardial strain for women and men were assessed.
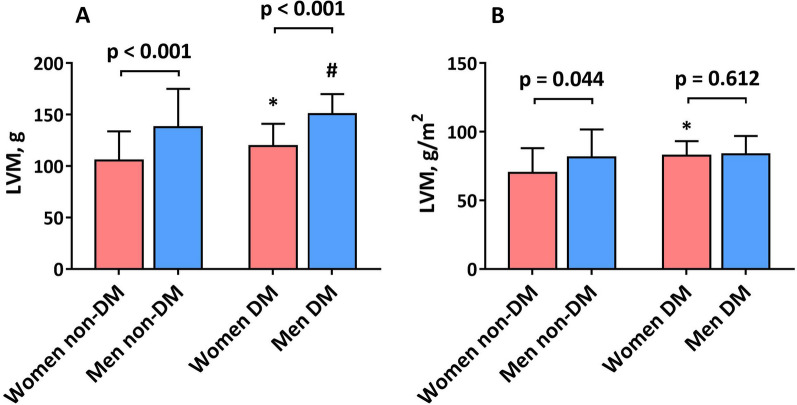
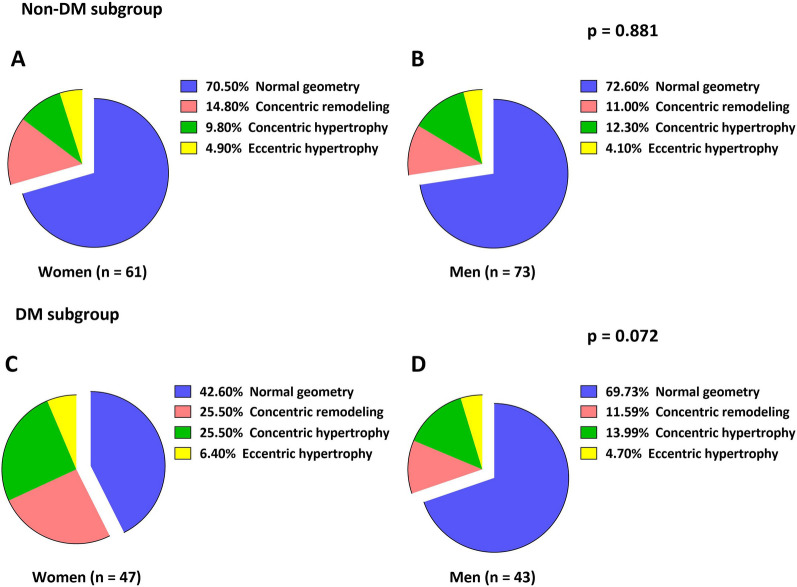
The prevalence of DM did not differ between sexes (p > 0.05). Despite a similar LV ejection fraction, women with DM demonstrated a greater LV mass index than women without DM (p = 0.023). The prevalence of LV geometry patterns by sex did not differ in the non-DM subgroup, but there was a trend toward a more abnormal LV geometry in women with DM (p = 0.072). The magnitudes of systolic strains were similar between sexes in the non-DM group (p > 0.05). Nevertheless, in the DM subgroup, there was significant impairment in women in systolic strains compared with men (p < 0.05). In the multivariable analysis, DM was associated with impaired systolic strains in women (GLS [β = 0.26; p = 0.007], GCS [β = 0.31; p < 0.001], and GRS [β = -0.24; p = 0.016]), whereas obesity and coronary artery disease were associated with impaired systolic strains in men (p < 0.05).
Women with DM demonstrated greater LV contractile dysfunction, which indicates that women with HFpEF comorbid with DM have a high-risk phenotype of cardiac failure that may require more aggressive and personalized medical treatment.
射血分数保留的心力衰竭(HFpEF)是一种具有性别特异性病理生理学的异质性综合征。雌激素缺乏被认为是女性 HFpEF 发展的原因。然而,雌激素缺乏似乎并不能完全解释男女 HFpEF 患病率的差异。虽然糖尿病(DM)在女性中常与 HFpEF 并存,并与预后更差相关,但 HFpEF 合并 DM 女性的心肌收缩力变化尚不清楚。因此,我们旨在研究 HFpEF 合并 DM 中与性别相关的左心室(LV)收缩功能障碍的差异。
本研究共纳入 224 例接受心脏电影磁共振成像(cine MRI)的患者。确定了 DM 背景下 LV 结构和功能的性别差异。使用 cine MRI 测量 LV 收缩期应变(整体纵向应变[GLS]、圆周应变[GCS]和径向应变[GRS])。评估了女性和男性心肌应变受损的决定因素。
DM 在性别间的患病率无差异(p>0.05)。尽管 LV 射血分数相似,但 DM 女性的 LV 质量指数大于无 DM 女性(p=0.023)。非 DM 亚组中,LV 几何形态的性别分布无差异,但 DM 女性的 LV 几何形态更异常(p=0.072)。非 DM 组中,男女间收缩期应变幅度无差异(p>0.05)。然而,DM 亚组中,女性的收缩期应变明显受损(p<0.05)。多变量分析显示,DM 与女性收缩期应变受损相关(GLS[β=0.26;p=0.007]、GCS[β=0.31;p<0.001]和 GRS[β=-0.24;p=0.016]),而肥胖和冠状动脉疾病与男性收缩期应变受损相关(p<0.05)。
DM 女性表现出更大的 LV 收缩功能障碍,这表明 HFpEF 合并 DM 的女性具有心力衰竭的高危表型,可能需要更积极和个性化的治疗。