Department of Family and Community Medicine, University of Toronto, Toronto, Canada.
Ray D. Wolfe Department of Family Medicine, Mount Sinai Hospital, Sinai Health, 60 Murray St, Toronto, ON, M5T 3L9, Canada.
BMC Fam Pract. 2021 Sep 15;22(1):185. doi: 10.1186/s12875-021-01536-3.
More than 90% of antibiotics are prescribed in primary care, but 50% may be unnecessary. Reducing unnecessary antibiotic overuse is needed to limit antimicrobial resistance. We conducted a pragmatic trial of a primary care provider-focused antimicrobial stewardship intervention to reduce antibiotic prescriptions in primary care.
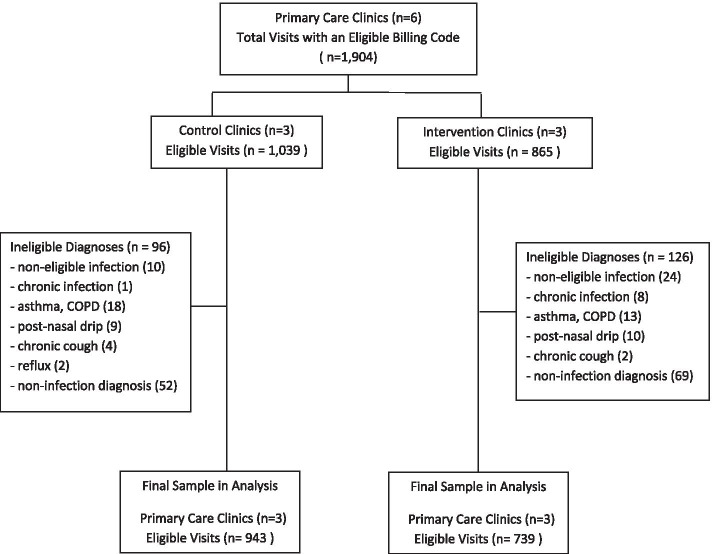
Primary care practitioners from six primary care clinics in Toronto, Ontario were assigned to intervention or control groups to evaluate the effectiveness of a multi-faceted intervention for reducing antibiotic prescriptions to adults with respiratory and urinary tract infections. The intervention included provider education, clinical decision aids, and audit and feedback of antibiotic prescribing. The primary outcome was total antibiotic prescriptions for these infections. Secondary outcomes were delayed prescriptions, prescriptions longer than 7 days, recommended antibiotic use, and outcomes for individual infections. Generalized estimating equations were used to estimate treatment effects, adjusting for clustering by clinic and baseline differences.
There were 1682 encounters involving 54 primary care providers from January until May 31, 2019. In intervention clinics, the odds of any antibiotic prescription was reduced 22% (adjusted Odds Ratio (OR) = 0.78; 95% Confidence Interval (CI) = 0.64.0.96). The odds that a delay in filling a prescription was recommended was increased (adjusted OR=2.29; 95% CI=1.37, 3.83), while prescription durations greater than 7 days were reduced (adjusted OR=0.24; 95% CI=0.13, 0.43). Recommended antibiotic use was similar in control (85.4%) and intervention clinics (91.8%, p=0.37).
A community-based, primary care provider-focused antimicrobial stewardship intervention was associated with a reduced likelihood of antibiotic prescriptions for respiratory and urinary infections, an increase in delayed prescriptions, and reduced prescription durations.
clinicaltrials.gov ( NCT03517215 ).
超过 90%的抗生素是在初级保健中开具的,但其中 50%可能是不必要的。为了限制抗菌药物耐药性的发生,需要减少不必要的抗生素过度使用。我们开展了一项以初级保健提供者为重点的抗菌药物管理干预措施的实用性试验,以减少初级保健中的抗生素处方。
安大略省多伦多市的六家初级保健诊所的初级保健医生被分配到干预组或对照组,以评估一种多方面的干预措施对减少成人呼吸道和尿路感染抗生素处方的有效性。该干预措施包括提供教育、临床决策辅助工具以及抗生素处方的审核和反馈。主要结局是这些感染的抗生素总处方量。次要结局是延迟处方、处方超过 7 天、推荐的抗生素使用以及个别感染的结局。使用广义估计方程估计治疗效果,调整诊所聚类和基线差异。
2019 年 1 月至 5 月 31 日,共涉及 54 名初级保健提供者的 1682 次就诊。在干预诊所,任何抗生素处方的可能性降低了 22%(调整后的优势比 (OR) = 0.78;95%置信区间 (CI) = 0.64.0.96)。建议延迟开处方的可能性增加(调整后的 OR=2.29;95% CI=1.37, 3.83),而 7 天以上的处方持续时间减少(调整后的 OR=0.24;95% CI=0.13, 0.43)。对照组(85.4%)和干预组(91.8%,p=0.37)推荐使用抗生素的情况相似。
以社区为基础、以初级保健提供者为重点的抗菌药物管理干预措施与呼吸道和尿路感染抗生素处方的可能性降低、延迟处方的增加以及处方持续时间的缩短有关。
clinicaltrials.gov(NCT03517215)。