MMWR Morb Mortal Wkly Rep. 2021 Sep 17;70(37):1267-1273. doi: 10.15585/mmwr.mm7037a1.
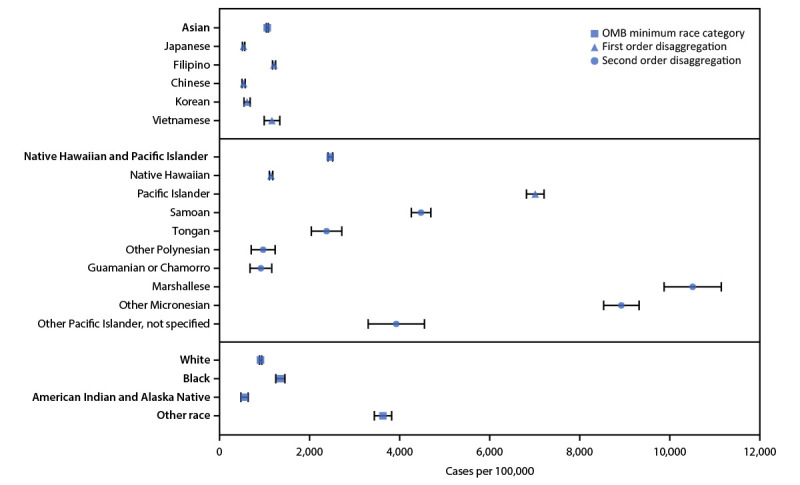
Native Hawaiian and Pacific Islander populations have been disproportionately affected by COVID-19 (1-3). Native Hawaiian, Pacific Islander, and Asian populations vary in language; cultural practices; and social, economic, and environmental experiences, which can affect health outcomes (4). However, data from these populations are often aggregated in analyses. Although data aggregation is often used as an approach to increase sample size and statistical power when analyzing data from smaller population groups, it can limit the understanding of disparities among diverse Native Hawaiian, Pacific Islander, and Asian subpopulations (4-7). To assess disparities in COVID-19 outcomes among Native Hawaiian, Pacific Islander, and Asian populations, a disaggregated, descriptive analysis, informed by recommendations from these communities,** was performed using race data from 21,005 COVID-19 cases and 449 COVID-19-associated deaths reported to the Hawaii State Department of Health (HDOH) during March 1, 2020-February 28, 2021. In Hawaii, COVID-19 incidence and mortality rates per 100,000 population were 1,477 and 32, respectively during this period. In analyses with race categories that were not mutually exclusive, including persons of one race alone or in combination with one or more races, Pacific Islander persons, who account for 5% of Hawaii's population, represented 22% of COVID-19 cases and deaths (COVID-19 incidence of 7,070 and mortality rate of 150). Native Hawaiian persons experienced an incidence of 1,181 and a mortality rate of 15. Among subcategories of Asian populations, the highest incidences were experienced by Filipino persons (1,247) and Vietnamese persons (1,200). Disaggregating Native Hawaiian, Pacific Islander, and Asian race data can aid in identifying racial disparities among specific subpopulations and highlights the importance of partnering with communities to develop culturally responsive outreach teams and tailored public health interventions and vaccination campaigns to more effectively address health disparities.
夏威夷原住民和太平洋岛民人口不成比例地受到 COVID-19 的影响 (1-3)。夏威夷原住民、太平洋岛民和亚裔人口在语言、文化习俗以及社会、经济和环境经历方面存在差异,这些差异会影响健康结果 (4)。然而,这些人群的数据通常在分析中汇总。虽然数据汇总通常被用作一种方法,以增加分析较小人群数据的样本量和统计能力,但它可能会限制对不同的夏威夷原住民、太平洋岛民和亚裔亚群之间差异的理解 (4-7)。为了评估 COVID-19 对夏威夷原住民、太平洋岛民和亚裔人口的影响,根据这些社区的建议,对 21,005 例 COVID-19 病例和 449 例与 COVID-19 相关的死亡报告进行了分类描述性分析,这些数据来自夏威夷州卫生署 (HDOH) 报告的 2020 年 3 月 1 日至 2021 年 2 月 28 日期间的 COVID-19 病例和死亡情况。在此期间,夏威夷每 100,000 人口的 COVID-19 发病率和死亡率分别为 1,477 和 32。在包括单独一种族或一种以上种族混合的种族类别相互不排斥的分析中,占夏威夷人口 5%的太平洋岛民占 COVID-19 病例和死亡人数的 22%(COVID-19 发病率为 7,070,死亡率为 150)。夏威夷原住民的发病率为 1,181,死亡率为 15。在亚裔人群的亚类中,菲律宾人 (1,247) 和越南人 (1,200) 的发病率最高。对夏威夷原住民、太平洋岛民和亚裔种族数据进行细分,可以帮助确定特定亚群中的种族差异,并强调与社区合作以组建具有文化响应能力的外展团队和制定针对性的公共卫生干预措施和疫苗接种运动的重要性,以更有效地解决健康差异问题。