Department of Neurology, University Medical Center Groningen, University of Groningen, Hanzeplein 1, PO Box 30.001, 9700 RB, Groningen, The Netherlands.
Department of Neurology, Philipps-Universität Marburg, Marburg, Germany.
Mol Med. 2021 Sep 16;27(1):111. doi: 10.1186/s10020-021-00327-x.
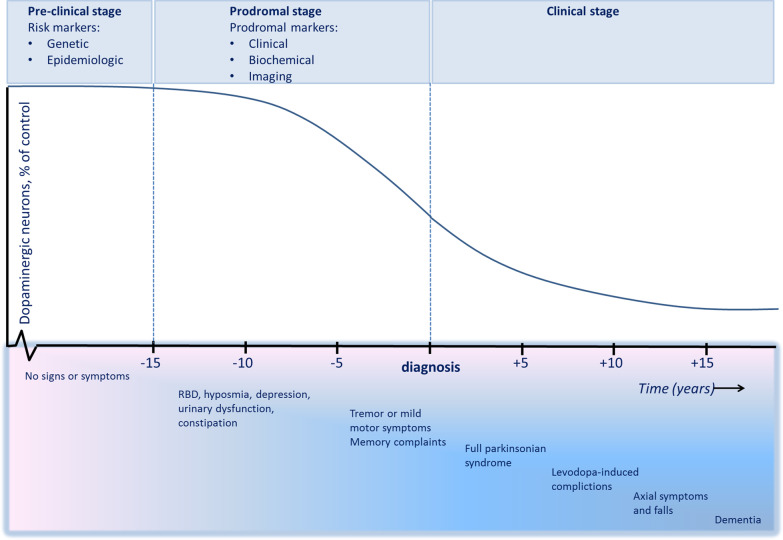
Parkinson's disease (PD) commences several years before the onset of motor features. Pathophysiological understanding of the pre-clinical or early prodromal stages of PD are essential for the development of new therapeutic strategies. Two categories of patients are ideal to study the early disease stages. Idiopathic rapid eye movement sleep behavior disorder (iRBD) represents a well-known prodromal stage of PD in which pathology is presumed to have reached the lower brainstem. The majority of patients with iRBD will develop manifest PD within years to decades. Another category encompasses non-manifest mutation carriers, i.e. subjects without symptoms, but with a known mutation or genetic variant which gives an increased risk of developing PD. The speed of progression from preclinical or prodromal to full clinical stages varies among patients and cannot be reliably predicted on the individual level. Clinical trials will require inclusion of patients with a predictable conversion within a limited time window. Biomarkers are necessary that can confirm pre-motor PD status and can provide information regarding lead time and speed of progression. Neuroimaging changes occur early in the disease process and may provide such a biomarker. Studies have focused on radiotracer imaging of the dopaminergic nigrostriatal system, which can be assessed with dopamine transporter (DAT) single photon emission computed tomography (SPECT). Loss of DAT binding represents an effect of irreversible structural damage to the nigrostriatal system. This marker can be used to monitor disease progression and identify individuals at specific risk for phenoconversion. However, it is known that changes in neuronal activity precede structural changes. Functional neuro-imaging techniques, such as F-2-fluoro-2-deoxy-D-glucose Positron Emission Tomography (F-FDG PET) and functional magnetic resonance imaging (fMRI), can be used to model the effects of disease on brain networks when combined with advanced analytical methods. Because these changes occur early in the disease process, functional imaging studies are of particular interest in prodromal PD diagnosis. In addition, fMRI and F-FDG PET may be able to predict a specific future phenotype in prodromal cohorts, which is not possible with DAT SPECT. The goal of the current review is to discuss the network-level brain changes in pre-motor PD.
帕金森病(PD)在运动症状出现前数年就开始了。对 PD 临床前或早期前驱期的病理生理学理解对于新的治疗策略的发展至关重要。有两类患者适合研究早期疾病阶段。特发性快速眼动睡眠行为障碍(iRBD)是 PD 的一个著名前驱阶段,在此阶段,病理被认为已经到达下脑。大多数 iRBD 患者将在数年内发展为明显的 PD。另一类包括非显性突变携带者,即无症状但具有已知突变或遗传变异的患者,这些变异会增加患 PD 的风险。从临床前或前驱期到完全临床期的进展速度在患者之间有所不同,无法在个体水平上可靠预测。临床试验将需要纳入在有限时间窗口内可预测转化的患者。需要有生物标志物来确认运动前期 PD 的状态,并提供关于潜伏期和进展速度的信息。神经影像学变化在疾病过程的早期发生,可能提供这样的生物标志物。研究集中在多巴胺能黑质纹状体系统的放射性示踪剂成像上,该系统可以用多巴胺转运蛋白(DAT)单光子发射计算机断层扫描(SPECT)进行评估。DAT 结合的丧失代表黑质纹状体系统不可逆结构损伤的影响。该标志物可用于监测疾病进展并识别具有特定表型转化风险的个体。然而,已知神经元活动的变化先于结构变化。功能神经影像学技术,如 F-2-氟-2-脱氧-D-葡萄糖正电子发射断层扫描(F-FDG PET)和功能磁共振成像(fMRI),与先进的分析方法结合使用时,可以用于模拟疾病对大脑网络的影响。由于这些变化发生在疾病过程的早期,因此功能成像研究在前驱性 PD 诊断中特别有趣。此外,fMRI 和 F-FDG PET 可能能够在前驱队列中预测特定的未来表型,而这是 DAT SPECT 无法做到的。本综述的目的是讨论运动前期 PD 的网络水平脑变化。