Department of Otolaryngology, Head and Neck Surgery, Rabin Medical Center - Beilinson Hospital, Petach Tikva, Israel; Sackler Faculty of Medicine, Tel Aviv University, Tel Aviv, Israel.
Department of Otolaryngology, Head and Neck Surgery, Rabin Medical Center - Beilinson Hospital, Petach Tikva, Israel.
Am J Otolaryngol. 2022 Jan-Feb;43(1):103230. doi: 10.1016/j.amjoto.2021.103230. Epub 2021 Sep 15.
Tracheostomy is an aerosol-generating procedure, thus performing it during the COVID-19 pandemic arises considerations such as the most appropriate timing and the patients to whom it is suitable. Medical teams lack sufficient data to assist determining whether or not to conduct tracheostomy, its short- and long-term implications are not fully understood. This study aims to shed light on the critically ill COVID-19 patients that require tracheostomy, and to investigate its value.
A retrospective multicentral case-control study of 157 hospitalized critically ill COVID-19 patients, among whom 30 patients went through tracheostomy and consisted of our study group.
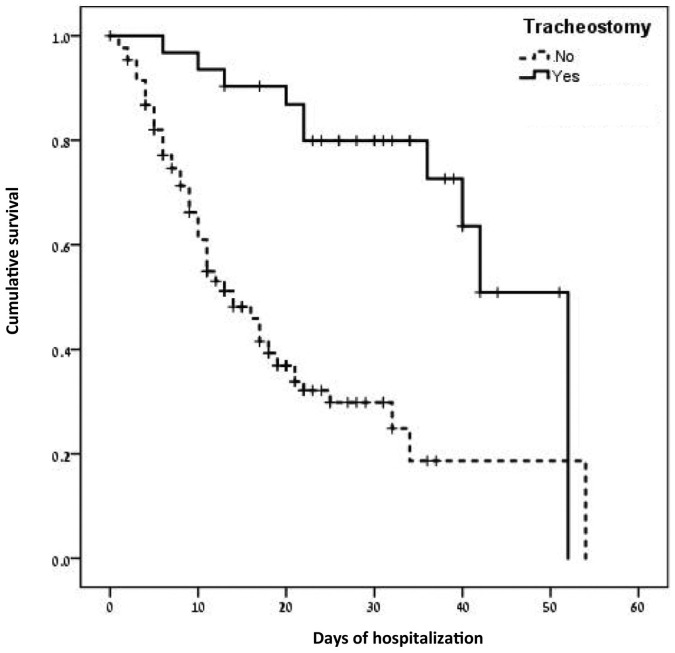
The mean age was similar between study and control groups (68.9 ± 12.7 years vs 70.5 ± 15.8 years, p = 0.57), as well as comorbidity prevalence (56.7% vs 67.7%, p = 0.25). Patients in the study group were hospitalized for longer duration until defined critically ill (5 ± 4.3 vs 3 ± 3.9 days; p = 0.01), until admitted to the intensive care unit (6 ± 6.6 vs 2.5 ± 3.7 days respectively; p = 0.005), and until discharged (24 ± 9.7 vs 10.7 ± 9.1 days, p < 0.001). Mortality rate was lower in the study group (30% vs 59.8%, p = 0.003). Kaplan Meier survival analysis revealed a statistically significant difference in survival time between groups (Log rank chi-sq = 20.91, p < 0.001) with mean survival time of 41 ± 3.1 days vs 21 ± 2.2 days. Survival was significantly longer in the study group (OR = 0.37, p = 0.004).
Tracheostomy allows for more prolonged survival for gradually deteriorating critically ill COVID-19 patients. This should be integrated into the medical teams' considerations when debating whether or not to conduct tracheostomy.
气管切开术是一种产生气溶胶的程序,因此在 COVID-19 大流行期间进行该手术需要考虑最适当的时机和适用的患者。医疗团队缺乏足够的数据来协助确定是否进行气管切开术,其短期和长期影响尚未完全了解。本研究旨在阐明需要气管切开术的危重症 COVID-19 患者,并探讨其价值。
对 157 名住院的危重症 COVID-19 患者进行回顾性多中心病例对照研究,其中 30 名患者接受了气管切开术,组成了我们的研究组。
研究组和对照组的平均年龄相似(68.9±12.7 岁 vs 70.5±15.8 岁,p=0.57),合并症患病率也相似(56.7% vs 67.7%,p=0.25)。研究组的患者在确定为危重症之前住院时间更长(5±4.3 天 vs 3±3.9 天;p=0.01),直到住进重症监护病房(6±6.6 天 vs 2.5±3.7 天;p=0.005),以及直到出院(24±9.7 天 vs 10.7±9.1 天,p<0.001)。研究组的死亡率较低(30% vs 59.8%,p=0.003)。Kaplan-Meier 生存分析显示两组之间的生存时间存在统计学差异(对数秩检验 chi-sq=20.91,p<0.001),研究组的平均生存时间为 41±3.1 天,而对照组为 21±2.2 天。研究组的生存时间显著延长(OR=0.37,p=0.004)。
气管切开术可使逐渐恶化的危重症 COVID-19 患者的生存时间更长。这应该纳入医疗团队在讨论是否进行气管切开术时的考虑因素。