Division of Pulmonary and Critical Care Medicine, Department of Medicine, New York University Langone Health, New York, New York; Department of Cardiothoracic Surgery, New York University Langone Health, New York, New York.
Department of Cardiothoracic Surgery, New York University Langone Health, New York, New York.
Ann Thorac Surg. 2020 Sep;110(3):1006-1011. doi: 10.1016/j.athoracsur.2020.04.010. Epub 2020 Apr 25.
Coronavirus 2019 (COVID-19) is a worldwide pandemic, with many patients requiring prolonged mechanical ventilation. Tracheostomy is not recommended by current guidelines as it is considered a superspreading event owing to aerosolization that unduly risks health care workers.
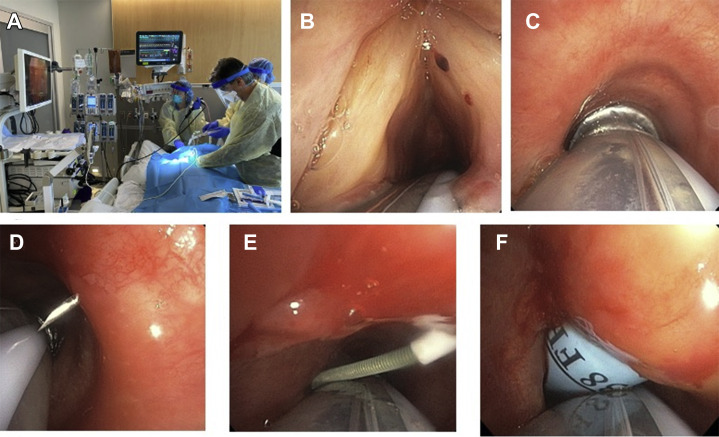
Patients with severe COVID-19 who were on mechanical ventilation for 5 days or longer were evaluated for percutaneous dilational tracheostomy. We developed a novel percutaneous tracheostomy technique that placed the bronchoscope alongside the endotracheal tube, not inside it. That improved visualization during the procedure and continued standard mechanical ventilation after positioning the inflated endotracheal tube cuff in the distal trachea. This technique offers a significant mitigation for the risk of virus aerosolization during the procedure.
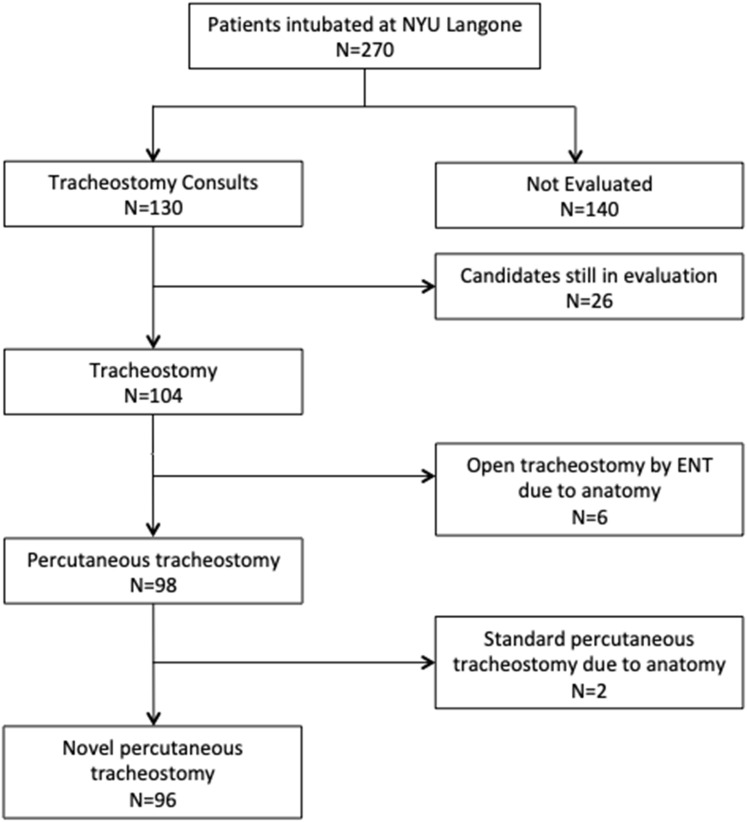
From March 10 to April 15, 2020, 270 patients with COVID-19 required invasive mechanical ventilation at New York University Langone Health Manhattan's campus; of those, 98 patients underwent percutaneous dilational tracheostomy. The mean time from intubation to the procedure was 10.6 ± 5 days. Currently, 32 patients (33%) do not require mechanical ventilatory support, 19 (19%) have their tracheostomy tube downsized, and 8 (8%) were decannulated. Forty patients (41%) remain on full ventilator support, and 19 (19%) are weaning from mechanical ventilation. Seven patients (7%) died as a result of respiratory and multiorgan failure. Tracheostomy-related bleeding was the most common complication (5 patients). None of health care providers has had symptoms or tested positive for COVID-19.
Our percutaneous tracheostomy technique appears to be safe and effective for COVID-19 patients and safe for health care workers.
2019 年冠状病毒病(COVID-19)是一场全球大流行,许多患者需要长时间接受机械通气。目前的指南不建议进行气管切开术,因为它被认为是一种超级传播事件,由于气溶胶化会对医护人员造成不必要的风险。
对机械通气 5 天或更长时间的重症 COVID-19 患者进行经皮扩张气管切开术评估。我们开发了一种新的经皮气管切开术技术,将支气管镜放在气管内导管旁边,而不是放在其内。这在将充气的气管内导管套囊定位在远端气管中后,改善了手术过程中的可视化效果,并继续进行标准的机械通气。该技术在手术过程中大大降低了病毒气溶胶化的风险。
2020 年 3 月 10 日至 4 月 15 日,纽约大学朗格尼健康曼哈顿校区有 270 名 COVID-19 患者需要进行有创机械通气;其中 98 名患者接受了经皮扩张气管切开术。从插管到手术的平均时间为 10.6 ± 5 天。目前,32 名患者(33%)不需要机械通气支持,19 名患者(19%)将气管切开管缩小,8 名患者(8%)拔管。40 名患者(41%)仍在接受全呼吸机支持,19 名患者(19%)正在从机械通气中脱机。7 名患者(7%)因呼吸和多器官衰竭而死亡。气管切开术相关出血是最常见的并发症(5 例)。没有医护人员出现症状或 COVID-19 检测呈阳性。
我们的经皮气管切开术技术似乎对 COVID-19 患者安全有效,对医护人员也安全。