IDAEA-CSIC, Barcelona, Catalonia, Spain.
Infectious Diseases Unit, Son Espases University Hospital, Palma, Mallorca, Spain; Balearic Islands Health Research Institute (IdISBa), Son Espases University Hospital, Palma, Mallorca, Spain.
Environ Res. 2022 Mar;204(Pt B):112074. doi: 10.1016/j.envres.2021.112074. Epub 2021 Sep 20.
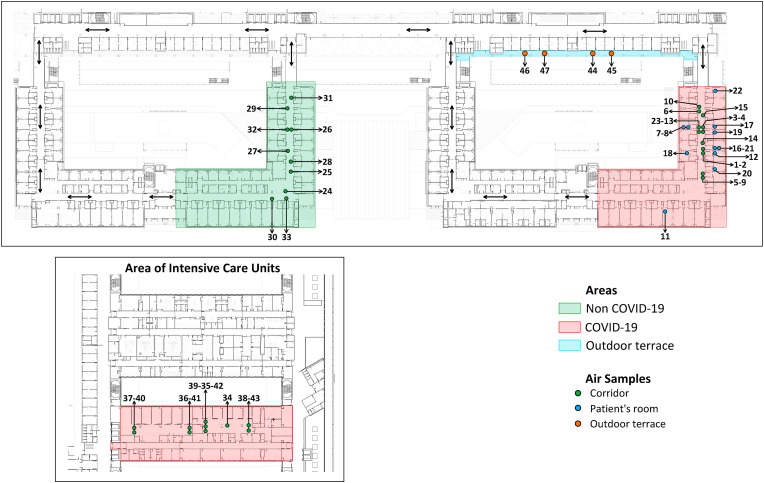
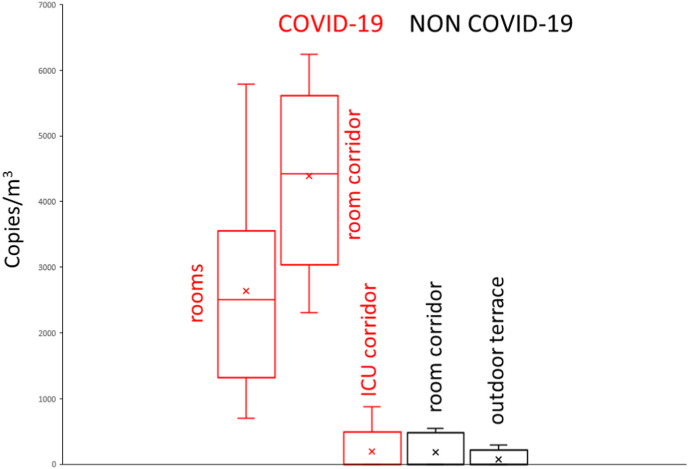
We performed a systematic sampling and analysis of airborne SARS-CoV-2 RNA in different hospital areas to assess viral spread. Systematic air filtration was performed in rooms with COVID-19 infected patients, in corridors adjacent to these rooms, to rooms of intensive care units, and to rooms with infected and uninfected patients, and in open spaces. RNA was extracted from the filters and real-time reverse transcription polymerase chain reaction was performed using the LightMix Modular SARS-CoV-2 E-gene. The highest occurrence of RNA was found in the rooms with COVID-19 patients (mean 2600 c/m) and the adjacent corridor (mean 4000 c/m) which was statistically significant more exposed (p < 0.01). This difference was related to the ventilation systems. As is commonly found in many hospitals, each of the rooms had an individual air inlet and outlet, while in the corridors these devices were located at the distance of every four rooms. There was a significant transfer of viruses from the COVID-19 patients' rooms to the corridors. The airborne SARS-CoV-2 RNA in the corridors of ICUs with COVID-19 patients or care rooms of uninfected patients were ten times lower, averages 190 c/m and 180 c/m, respectively, without presenting significant differences. In all COVID-19 ICU rooms, patients were intubated and connected to respirators that filtered all exhaled air and prevented virus release, resulting in significantly lower viral concentrations in adjacent corridors. The results show that the greatest risk of nosocomial infection may also occur in hospital areas not directly exposed to the exhaled breath of infected patients. Hospitals should evaluate the ventilation systems of all units to minimize possible contagion and, most importantly, direct monitoring of SARS-CoV-2 in the air should be carried out to prevent unexpected viral exposures.
我们对不同医院区域的空气传播 SARS-CoV-2 RNA 进行了系统采样和分析,以评估病毒传播情况。在感染 COVID-19 的患者所在的房间、这些房间相邻的走廊、重症监护病房的房间以及感染和未感染患者的房间以及开放空间中进行了系统空气过滤。从过滤器中提取 RNA,并使用 LightMix 模块化 SARS-CoV-2 E 基因进行实时逆转录聚合酶链反应。在感染 COVID-19 的患者的房间(平均值 2600 c/m)和相邻的走廊(平均值 4000 c/m)中发现 RNA 的发生率最高,这在统计学上是显著更高的暴露(p < 0.01)。这种差异与通风系统有关。与许多医院常见的情况一样,每个房间都有一个单独的进风口和出风口,而在走廊中,这些设备位于每四个房间的距离处。病毒从 COVID-19 患者的房间转移到走廊的情况非常明显。感染 COVID-19 的患者的 ICU 走廊或未感染患者的护理室中的空气传播 SARS-CoV-2 RNA 分别低十倍,平均值为 190 c/m 和 180 c/m,没有呈现出显著差异。在所有 COVID-19 ICU 房间中,患者都被插管并连接到呼吸机,呼吸机过滤所有呼出的空气并防止病毒释放,从而导致相邻走廊中的病毒浓度显著降低。结果表明,医院区域中最有可能发生医院感染的风险也可能发生在未直接暴露于感染患者呼出物的区域。医院应评估所有单位的通风系统,以最大程度地减少可能的传染,最重要的是,应进行空气中 SARS-CoV-2 的直接监测,以防止意外的病毒暴露。