Bass E J, Pantovic A, Connor M J, Loeb S, Rastinehad A R, Winkler M, Gabe Rhian, Ahmed H U
Imperial Prostate. Division of Surgery, Department of Surgery and Cancer, Faculty of Medicine, Imperial College London, London, UK.
Imperial Urology, Division of Cancer, Cardiovascular Medicine and Surgery, Imperial College Healthcare NHS Trust, London, UK.
Prostate Cancer Prostatic Dis. 2022 Feb;25(2):174-179. doi: 10.1038/s41391-021-00449-7. Epub 2021 Sep 21.
Multiparametric MRI localizes cancer in the prostate, allowing for MRI guided biopsy (MRI-GB) 43 alongside transrectal ultrasound-guided systematic biopsy (TRUS-GB). Three MRI-GB approaches exist; visual estimation (COG-TB); fusion software-assisted (FUS-TB) and MRI 'in-bore' biopsy (IB-TB). It is unknown whether any of these are superior. We conducted a systematic review and meta-analysis to address three questions. First, whether MRI-GB is superior to TRUS-GB at detecting clinically significant PCa (csPCa). Second, whether MRI-GB is superior to TRUS-GB at avoiding detection of insignificant PCa. Third, whether any MRI-GB strategy is superior at detecting csPCa.
A systematic literature review from 2015 to 2019 was performed in accordance with the START recommendations. Studies reporting PCa detection rates, employing MRI-GB and TRUS-GB were included and evaluated using the QUADAS-2 checklist. 1553 studies were found, of which 43 were included in the meta-analysis.
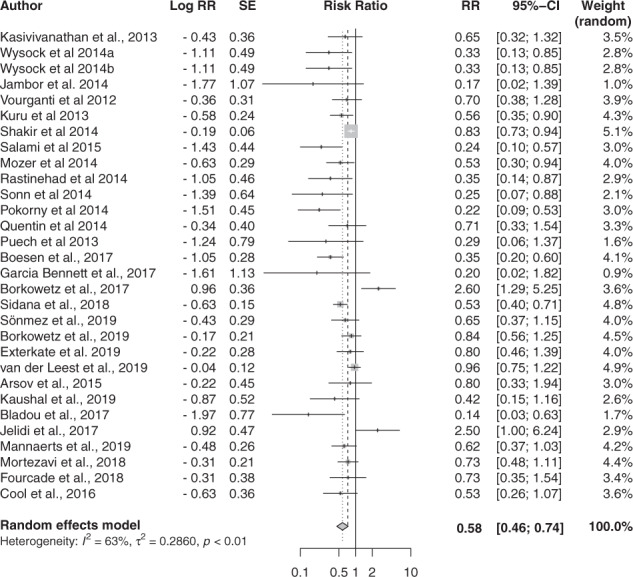
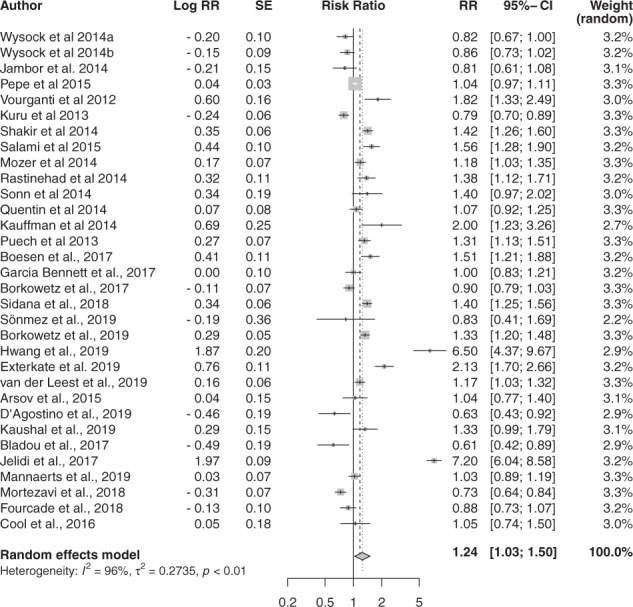
For csPCa, MRI-GB was superior in detection to TRUS-GB (0.83 vs. 0.63 [p = 0.02]). MRI-GB was superior in detection to TRUS-GB at avoiding detection of insignificant PCa. No MRI-GB technique was superior at detecting csPCa (IB-TB 0.87; COG TB 0.81; FUS-TB 0.81, [p = 0.55]). There was significant heterogeneity observed between the included studies.
In patients with suspected PCa on MRI, MRI-GB offers superior rates of csPCa detection and reduces detection of insignificant PCa compared to TRUS-GB. No individual MRI-GB technique was found to be better in csPCa detection. Prospective adequately powered randomized controlled trials are required.
多参数磁共振成像(MRI)可对前列腺癌进行定位,从而实现MRI引导下的活检(MRI-GB),同时还可进行经直肠超声引导下的系统活检(TRUS-GB)。目前存在三种MRI引导下活检的方法:视觉估计法(COG-TB);融合软件辅助法(FUS-TB)和MRI“孔内”活检法(IB-TB)。尚不清楚这些方法中是否有哪一种更具优势。我们进行了一项系统评价和荟萃分析,以回答三个问题。第一,在检测临床显著性前列腺癌(csPCa)方面,MRI引导下活检是否优于经直肠超声引导下活检。第二,在避免检测到非显著性前列腺癌方面,MRI引导下活检是否优于经直肠超声引导下活检。第三,在检测临床显著性前列腺癌方面,是否有任何一种MRI引导下活检策略更具优势。
根据START建议,对2015年至2019年的文献进行了系统回顾。纳入报告采用MRI引导下活检和经直肠超声引导下活检的前列腺癌检测率的研究,并使用QUADAS-2清单进行评估。共检索到1553项研究,其中43项纳入荟萃分析。
对于临床显著性前列腺癌,MRI引导下活检在检测方面优于经直肠超声引导下活检(0.83对0.63 [p = 0.02])。在避免检测到非显著性前列腺癌方面,MRI引导下活检在检测方面优于经直肠超声引导下活检。在检测临床显著性前列腺癌方面,没有一种MRI引导下活检技术更具优势(IB-TB 0.87;COG TB 0.81;FUS-TB 0.81,[p = 0.55])。纳入的研究之间观察到显著的异质性。
对于MRI检查怀疑患有前列腺癌的患者,与经直肠超声引导下活检相比,MRI引导下活检在检测临床显著性前列腺癌方面具有更高的检出率,并减少了非显著性前列腺癌的检测。在检测临床显著性前列腺癌方面,未发现哪种单独的MRI引导下活检技术更优。需要进行前瞻性、有足够样本量的随机对照试验。