Pinter Zachariah W, Reed Ryder, Townsley Sarah E, Mikula Anthony L, Dittman Lauren, Xiong Ashley, Skjaerlund Jonathan, Michalopoulos Giorgos D, Currier Bradford, Nassr Ahmad, Fogelson Jeremy L, Freedman Brett A, Bydon Mohamad, Kepler Christopher K, Wagner Scott C, Elder Benjamin D, Sebastian Arjun S
Department of Orthopedic Surgery, Mayo Clinic, Rochester, MN, USA.
Department of Neurologic Surgery, Mayo Clinic, Rochester, MN, USA.
Global Spine J. 2023 Sep;13(7):1703-1715. doi: 10.1177/21925682211046897. Epub 2021 Sep 24.
Retrospective cohort study.
Substantial variability in both the measurement and classification of subsidence limits the strength of conclusions that can be drawn from previous studies. The purpose of this study was to precisely characterize patterns of cervical cage subsidence utilizing computed tomography (CT) scans, determine risk factors for cervical cage subsidence, and investigate the impact of subsidence on pseudarthrosis rates.
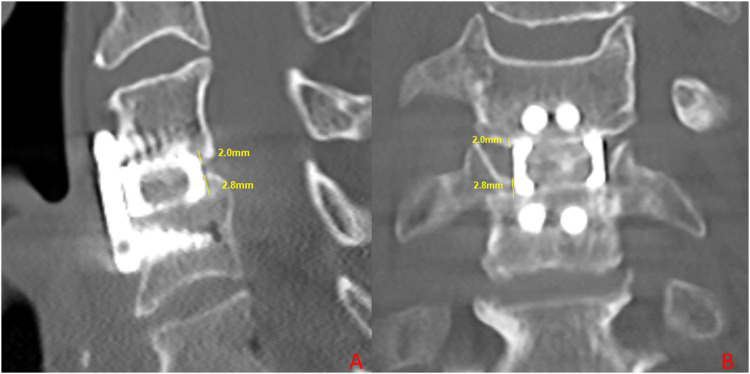
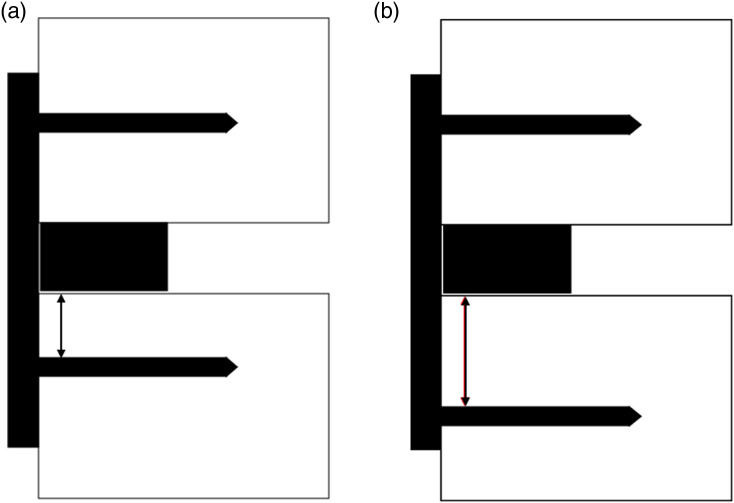
We performed a retrospective review of patients who underwent one- to three-levels of anterior cervical discectomy and fusion (ACDF) utilizing titanium interbodies with anterior plating between the years 2018 and 2020. Subsidence measurements were performed by two independent reviewers on CT scans obtained 6 months postoperatively. Subsidence was then classified as mild if subsidence into the inferior and superior endplate were both ≤2 mm, moderate if the worst subsidence into the inferior or superior endplate was between 2 to 4 mm, or severe if the worst subsidence into the inferior or superior endplate was ≥4 mm.
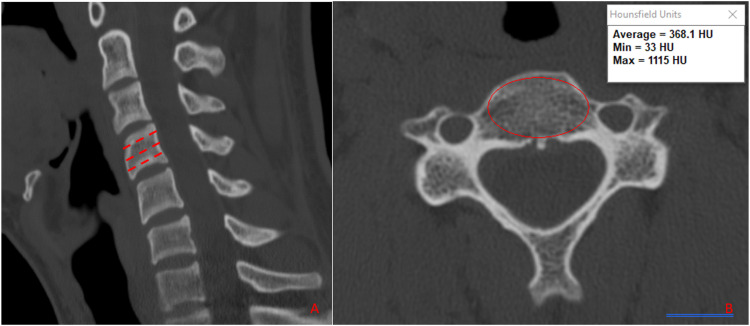
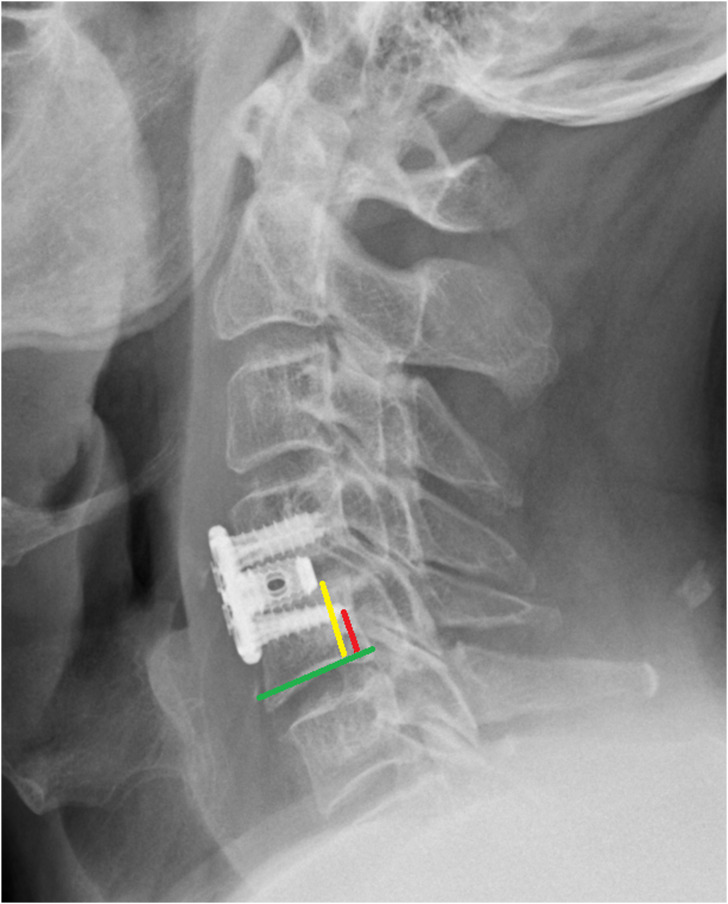
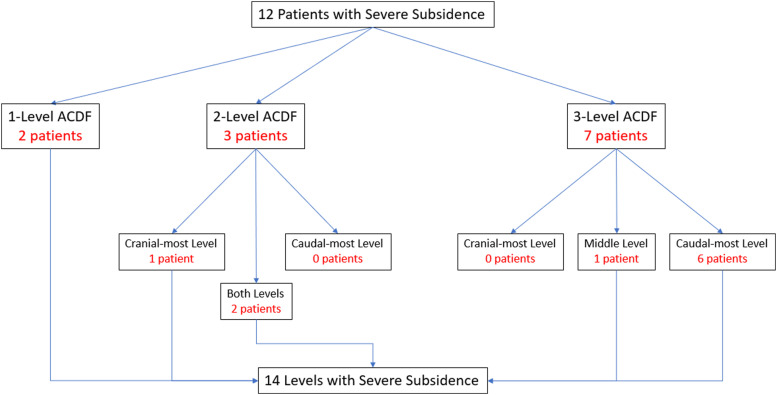
A total of 51 patients (100 levels) were included in this study. A total of 48 levels demonstrated mild subsidence (≤2 mm), 38 demonstrated moderate subsidence (2-4 mm), and 14 demonstrated severe subsidence (≥4 mm). Risk factors for severe subsidence included male gender, multilevel constructs, greater mean vertebral height loss, increased cage height, lower Taillard index, and lower screw tip to vertebral body height ratio. Severe subsidence was not associated with an increased rate of pseudarthrosis.
Following ACDF with titanium cervical cages, subsidence is an anticipated postoperative occurrence and is not associated with an increased risk of pseudarthrosis.
回顾性队列研究。
下沉的测量和分类存在很大差异,这限制了从先前研究中得出结论的力度。本研究的目的是利用计算机断层扫描(CT)精确描述颈椎椎间融合器下沉的模式,确定颈椎椎间融合器下沉的危险因素,并研究下沉对假关节形成率的影响。
我们对2018年至2020年间接受一至三节段前路颈椎间盘切除融合术(ACDF)并使用钛制椎间融合器和前路钢板固定的患者进行了回顾性研究。由两名独立的评估人员对术后6个月获得的CT扫描进行下沉测量。如果椎间融合器向上下终板的下沉均≤2mm,则下沉分类为轻度;如果向上下终板的最大下沉在2至4mm之间,则为中度;如果向上下终板的最大下沉≥4mm,则为重度。
本研究共纳入51例患者(100个节段)。共有48个节段表现为轻度下沉(≤2mm),38个节段表现为中度下沉(2 - 4mm),14个节段表现为重度下沉(≥4mm)。重度下沉的危险因素包括男性、多节段结构、平均椎体高度丢失更大、椎间融合器高度增加、Taillard指数较低以及螺钉尖端与椎体高度比值较低。重度下沉与假关节形成率增加无关。
使用钛制颈椎椎间融合器进行ACDF术后,下沉是一种预期的术后现象,且与假关节形成风险增加无关。