Department of Internal Medicine, Division of Cardiology, Kangnam Sacred Heart Hospital, Hallym University College of Medicine, Beodeunaru-ro 7-gil, Yeongdeungpo-gu, Seoul 07247, Korea.
Department of Cardiothoracic Surgery, Kangnam Sacred Heart Hospital, Hallym University College of Medicine, Seoul 07247, Korea.
Medicina (Kaunas). 2021 Aug 27;57(9):886. doi: 10.3390/medicina57090886.
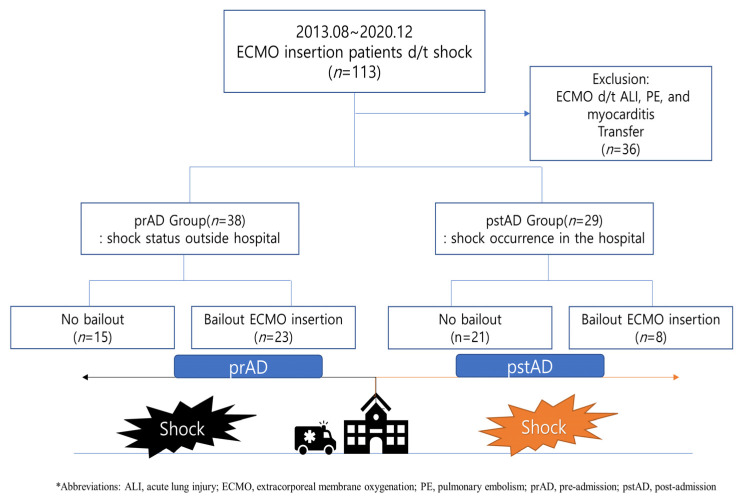
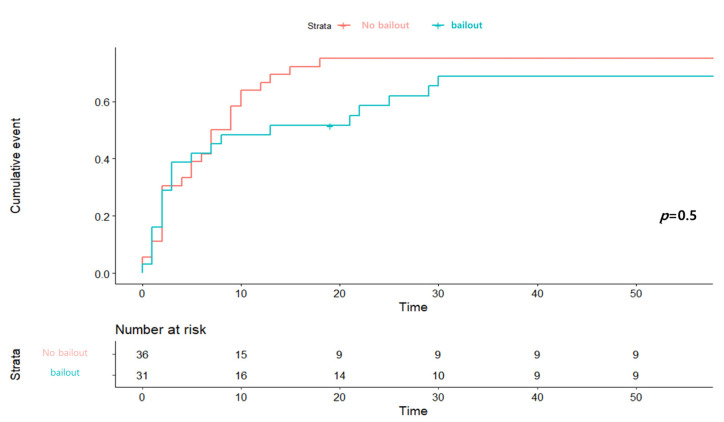
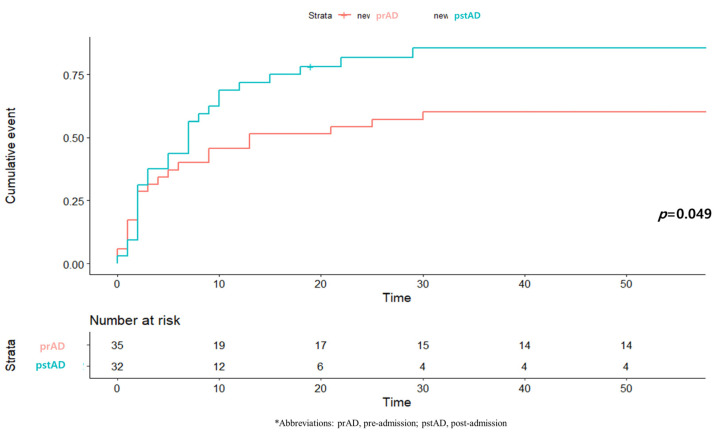
Extracorporeal membrane oxygenation (ECMO) can be helpful in patients with cardiogenic shock associated with myocardial infarction, and its early use can improve the patient survival rate. In this study, we report a mortality rate-difference analysis that examined the time and location of shock occurrence. We enrolled patients who underwent ECMO due to cardiogenic shock related to myocardial infarction and assigned them to either a pre- or post-admission shock group. The primary outcome was the 1-month mortality rate; a subgroup analysis was conducted to assess the effect of bailout ECMO. Of the 113 patients enrolled, 67 (38 with pre-admission shock, 29 with post-admission shock) were analysed. Asystole was more frequently detected in the pre-admission shock group than in the post-admission group. In both groups, the commonest culprit lesion location was in the left anterior descending artery. Cardiopulmonary resuscitation was performed significantly more frequently and earlier in the pre-admission group. The 1-month mortality rate was significantly lower in the pre-admission group than in the post-admission group. Male sex and ECMO duration (≥6 days) were factors significantly related to the reduced mortality rate in the pre-admission group. In the subgroup analysis, the mortality rate was lower in patients receiving bailout ECMO than in those not receiving it; the difference was not statistically significant. ECMO application resulted in lower short-term mortality rate among patients with out-of-hospital cardiogenic shock onset than with in-hospital shock onset; early cardiopulmonary resuscitation and ECMO might be helpful in select patients.
体外膜肺氧合(ECMO)可用于治疗与心肌梗死相关的心源性休克患者,早期应用可提高患者的生存率。在这项研究中,我们报告了一项死亡率差异分析,该分析检查了休克发生的时间和地点。我们招募了因心肌梗死导致心源性休克而接受 ECMO 治疗的患者,并将其分为入院前休克组或入院后休克组。主要结局是 1 个月死亡率;进行了亚组分析以评估挽救性 ECMO 的效果。在纳入的 113 例患者中,有 67 例(38 例入院前休克,29 例入院后休克)进行了分析。在入院前休克组中,更常检测到心搏停止。在两组中,最常见的罪犯病变部位均在左前降支。入院前休克组心肺复苏的实施明显更频繁且更早。入院前休克组的 1 个月死亡率明显低于入院后休克组。男性和 ECMO 持续时间(≥6 天)是入院前休克组死亡率降低的显著相关因素。在亚组分析中,接受挽救性 ECMO 的患者死亡率低于未接受者,但差异无统计学意义。ECMO 的应用可降低院外心源性休克发作患者的短期死亡率,而院内休克发作患者的死亡率则较高;早期心肺复苏和 ECMO 可能对某些患者有帮助。