Department of Cardiovascular Surgery, Mayo Clinic, Rochester, MN 55905, USA.
Division of Pediatric Critical Care Medicine, Department of Pediatrics, Stanford University School of Medicine, Stanford, CA 94305, USA.
Medicina (Kaunas). 2021 Sep 2;57(9):926. doi: 10.3390/medicina57090926.
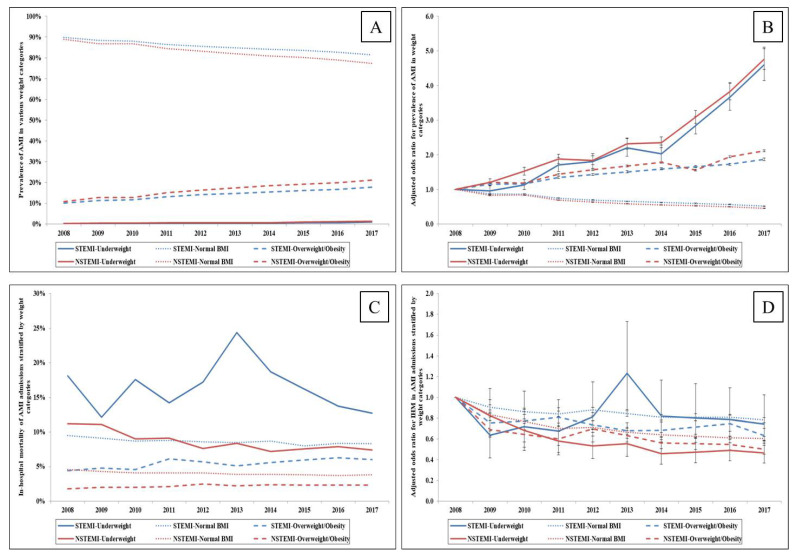
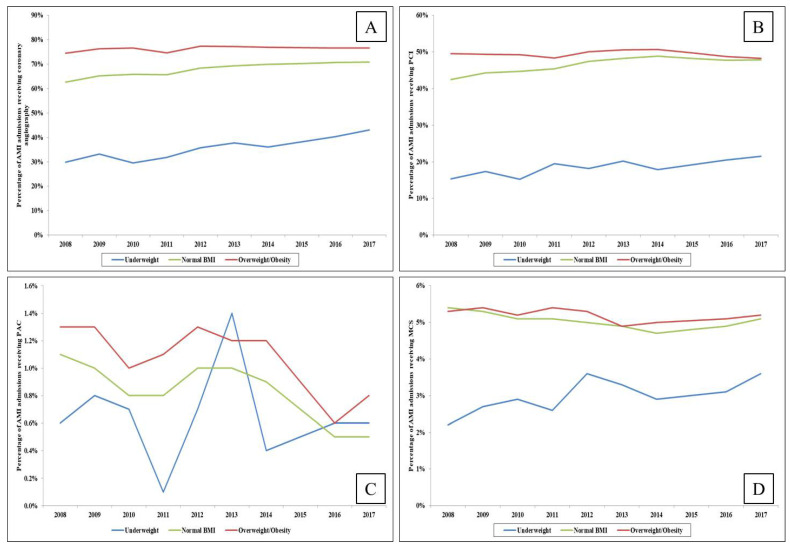
: Contemporary data on the prevalence, management and outcomes of acute myocardial infarction (AMI) in relation to body mass index (BMI) are limited. : Using the National Inpatient Sample from 2008 through 2017, we identified adult AMI hospitalizations and categorized them into underweight (BMI < 19.9 kg/m), normal BMI and overweight/obese (BMI > 24.9 kg/m) groups. We evaluated in-hospital mortality, utilization of cardiac procedures and resource utilization among these groups. : Among 6,089,979 admissions for AMI, 38,070 (0.6%) were underweight, 5,094,721 (83.7%) had normal BMI, and 957,188 (15.7%) were overweight or obese. Over the study period, an increase in the prevalence of AMI was observed in underweight and overweight/obese admissions. Underweight AMI admissions were, on average, older, with higher comorbidity, whereas overweight/obese admissions were younger and had lower comorbidity. In comparison to the normal BMI and overweight/obese categories, significantly lower use of coronary angiography (62.3% vs. 74.6% vs. 37.9%) and PCI (40.8% vs. 47.7% vs. 19.6%) was observed in underweight admissions (all < 0.001). The underweight category was associated with significantly higher in-hospital mortality (10.0% vs. 5.5%; OR 1.23 (95% CI 1.18-1.27), < 0.001), whereas being overweight/obese was associated with significantly lower in-hospital mortality compared to normal BMI admissions (3.1% vs. 5.5%; OR 0.73 (95% CI 0.72-0.74), < 0.001). Underweight AMI admissions had longer lengths of in-hospital stay with frequent discharges to skilled nursing facilities, while overweight/obese admissions had higher hospitalization costs. : In-hospital management and outcomes of AMI vary by BMI. Underweight status was associated with worse outcomes, whereas the obesity paradox was apparent, with better outcomes for overweight/obese admissions.
目前关于与体重指数(BMI)相关的急性心肌梗死(AMI)的患病率、治疗方法和结局的数据较为有限。利用 2008 年至 2017 年的国家住院患者样本,我们确定了成人 AMI 住院患者,并将其分为体重不足(BMI<19.9kg/m)、正常 BMI 和超重/肥胖(BMI>24.9kg/m)组。我们评估了这些组别的住院死亡率、心脏手术的使用情况和资源利用情况。在 6089979 例 AMI 住院患者中,38070 例(0.6%)体重不足,5094721 例(83.7%)BMI 正常,957188 例(15.7%)超重或肥胖。在研究期间,体重不足和超重/肥胖入院的 AMI 患病率均有所增加。体重不足的 AMI 入院患者平均年龄较大,合并症较多,而超重/肥胖的 AMI 入院患者年龄较小,合并症较少。与 BMI 正常和超重/肥胖组相比,体重不足组的冠状动脉造影(62.3% vs. 74.6% vs. 37.9%)和经皮冠状动脉介入治疗(PCI)(40.8% vs. 47.7% vs. 19.6%)使用率显著降低(均<0.001)。体重不足组的住院死亡率显著较高(10.0% vs. 5.5%;OR 1.23(95%CI 1.18-1.27),<0.001),而超重/肥胖组与 BMI 正常组相比,住院死亡率显著较低(3.1% vs. 5.5%;OR 0.73(95%CI 0.72-0.74),<0.001)。体重不足的 AMI 入院患者的住院时间较长,常被转至康复护理机构,而超重/肥胖的 AMI 入院患者的住院费用较高。AMI 的院内管理和结局因 BMI 而异。体重不足与较差的结局相关,而肥胖悖论明显,超重/肥胖的入院患者有更好的结局。