Department of Anaesthesiology, Intensive Care and Pain Medicine, University of Helsinki and Helsinki University Hospital, Meilahden SairaalaHaartmaninkatu 4, 000290, Helsinki, Finland.
Intensive Care Unit, Liverpool Hospital, South Western Sydney Local Health District, Sydney, Australia.
Crit Care. 2021 Sep 28;25(1):350. doi: 10.1186/s13054-021-03764-6.
Impaired cerebrovascular reactivity (CVR) is one feature of post cardiac arrest encephalopathy. We studied the incidence and features of CVR by near infrared spectroscopy (NIRS) and associations with outcome and biomarkers of brain injury.
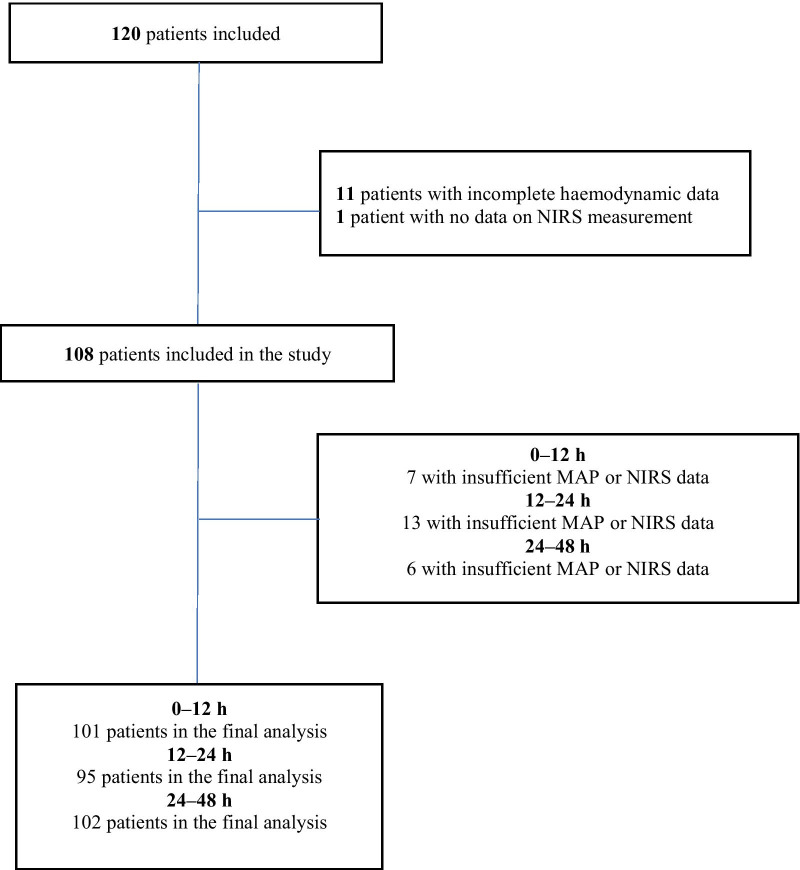
A post-hoc analysis of 120 comatose OHCA patients continuously monitored with NIRS and randomised to low- or high-normal oxygen, carbon dioxide and mean arterial blood pressure (MAP) targets for 48 h. The tissue oximetry index (TO) generated by the moving correlation coefficient between cerebral tissue oxygenation measured by NIRS and MAP was used as a dynamic index of CVR with TO > 0 indicating impaired reactivity and TO > 0.3 used to delineate the lower and upper MAP bounds for disrupted CVR. TO was analysed in the 0-12, 12-24, 24-48 h time-periods and integrated over 0-48 h. The primary outcome was the association between TO and six-month functional outcome dichotomised by the cerebral performance category (CPC1-2 good vs. 3-5 poor). Secondary outcomes included associations with MAP bounds for CVR and biomarkers of brain injury.
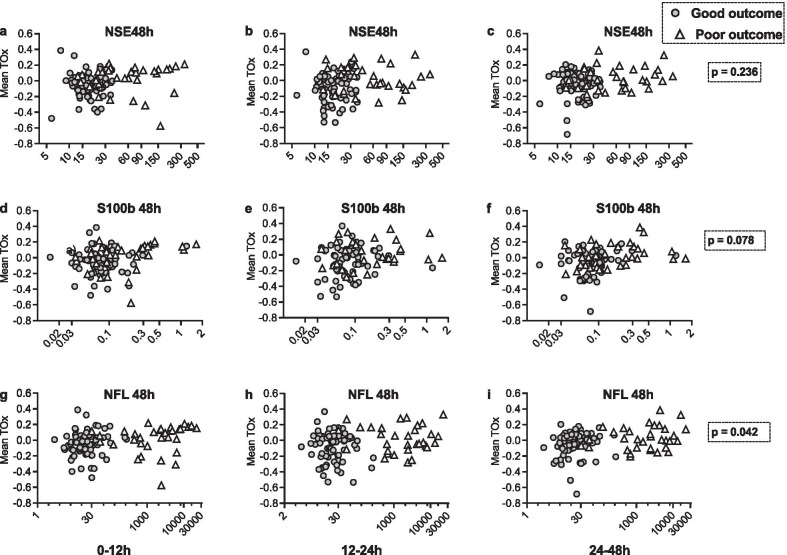
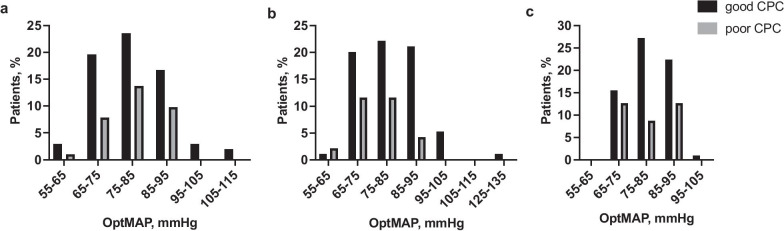
In 108 patients with sufficient data to calculate TO, 76 patients (70%) had impaired CVR and among these, chronic hypertension was more common (58% vs. 31%, p = 0.002). Integrated TO for 0-48 h was higher in patients with poor outcome than in patients with good outcome (0.89 95% CI [- 1.17 to 2.94] vs. - 2.71 95% CI [- 4.16 to - 1.26], p = 0.05). Patients with poor outcomes had a decreased upper MAP bound of CVR over time (p = 0.001), including the high-normal oxygen (p = 0.002), carbon dioxide (p = 0.012) and MAP (p = 0.001) groups. The MAP range of maintained CVR was narrower in all time intervals and intervention groups (p < 0.05). NfL concentrations were higher in patients with impaired CVR compared to those with intact CVR (43 IQR [15-650] vs 20 IQR [13-199] pg/ml, p = 0.042).
Impaired CVR over 48 h was more common in patients with chronic hypertension and associated with poor outcome. Decreased upper MAP bound and a narrower MAP range for maintained CVR were associated with poor outcome and more severe brain injury assessed with NfL. Trial registration ClinicalTrials.gov, NCT02698917 .
脑卒中心跳骤停后患者的脑血管反应性(CVR)受损是一种特征。我们通过近红外光谱(NIRS)研究了 CVR 的发生率和特征,以及与预后和脑损伤生物标志物的关系。
这是一项对 120 例连续接受 NIRS 监测并随机分为低或高正常氧、二氧化碳和平均动脉血压(MAP)目标 48 小时的心脏骤停后昏迷患者的事后分析。通过 NIRS 测量的脑组织氧合与 MAP 之间的移动相关系数生成的组织血氧指数(TO)被用作 CVR 的动态指标,TO>0 表示反应受损,TO>0.3 用于描绘受损 CVR 的下限和上限 MAP 边界。在 0-12、12-24 和 24-48 小时时间段内分析 TO,并在 0-48 小时期间进行积分。主要结局是 TO 与 6 个月时功能结局(通过脑功能分类 CPC1-2 良好与 3-5 不良划分)之间的相关性。次要结局包括与 CVR 的 MAP 边界和脑损伤生物标志物的相关性。
在 108 例有足够数据计算 TO 的患者中,76 例(70%)患者存在 CVR 受损,其中慢性高血压更为常见(58%比 31%,p=0.002)。0-48 小时的综合 TO 在预后不良的患者中高于预后良好的患者(0.89 95%CI [-1.17 至 2.94] 比 -2.71 95%CI [-4.16 至 -1.26],p=0.05)。预后不良的患者随着时间的推移 CVR 的上限 MAP 边界降低(p=0.001),包括高正常氧(p=0.002)、二氧化碳(p=0.012)和 MAP(p=0.001)组。所有时间间隔和干预组中,维持 CVR 的 MAP 范围更窄(p<0.05)。与 CVR 正常的患者相比,CVR 受损的患者神经丝轻链(NfL)浓度更高(43 IQR [15-650] 比 20 IQR [13-199] pg/ml,p=0.042)。
48 小时内 CVR 受损在患有慢性高血压的患者中更为常见,与不良预后相关。CVR 上限 MAP 边界降低和维持 CVR 的 MAP 范围变窄与预后不良和使用 NfL 评估的更严重脑损伤相关。
ClinicalTrials.gov,NCT02698917。