Department of Epidemiology and Biostatistics, Medicine, UCSF, San Francisco, CA (A.L.B.).
Department of Medicine, University of Alabama, Birmingham (T.M.B.).
Circ Cardiovasc Qual Outcomes. 2021 Oct;14(10):e008215. doi: 10.1161/CIRCOUTCOMES.121.008215. Epub 2021 Sep 30.
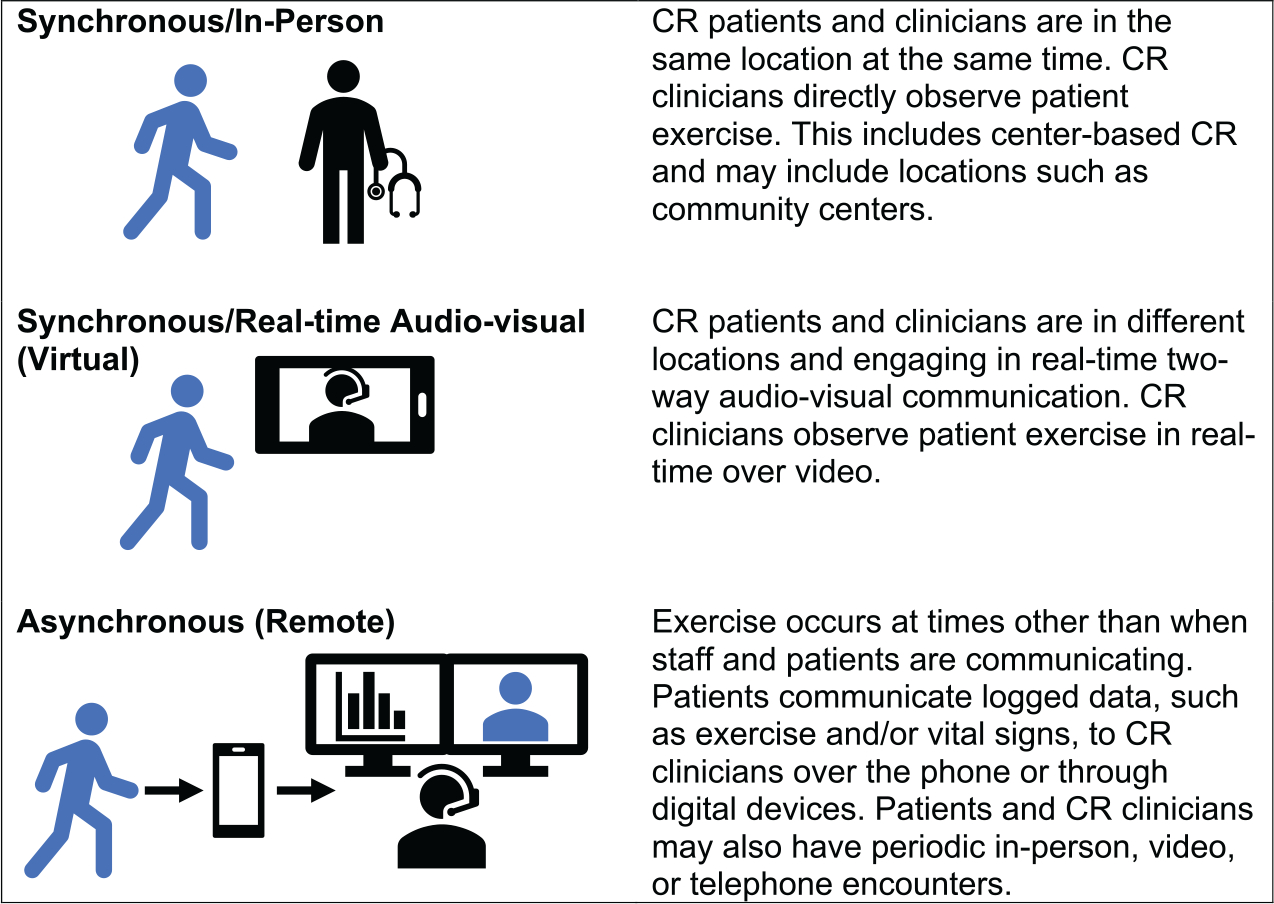
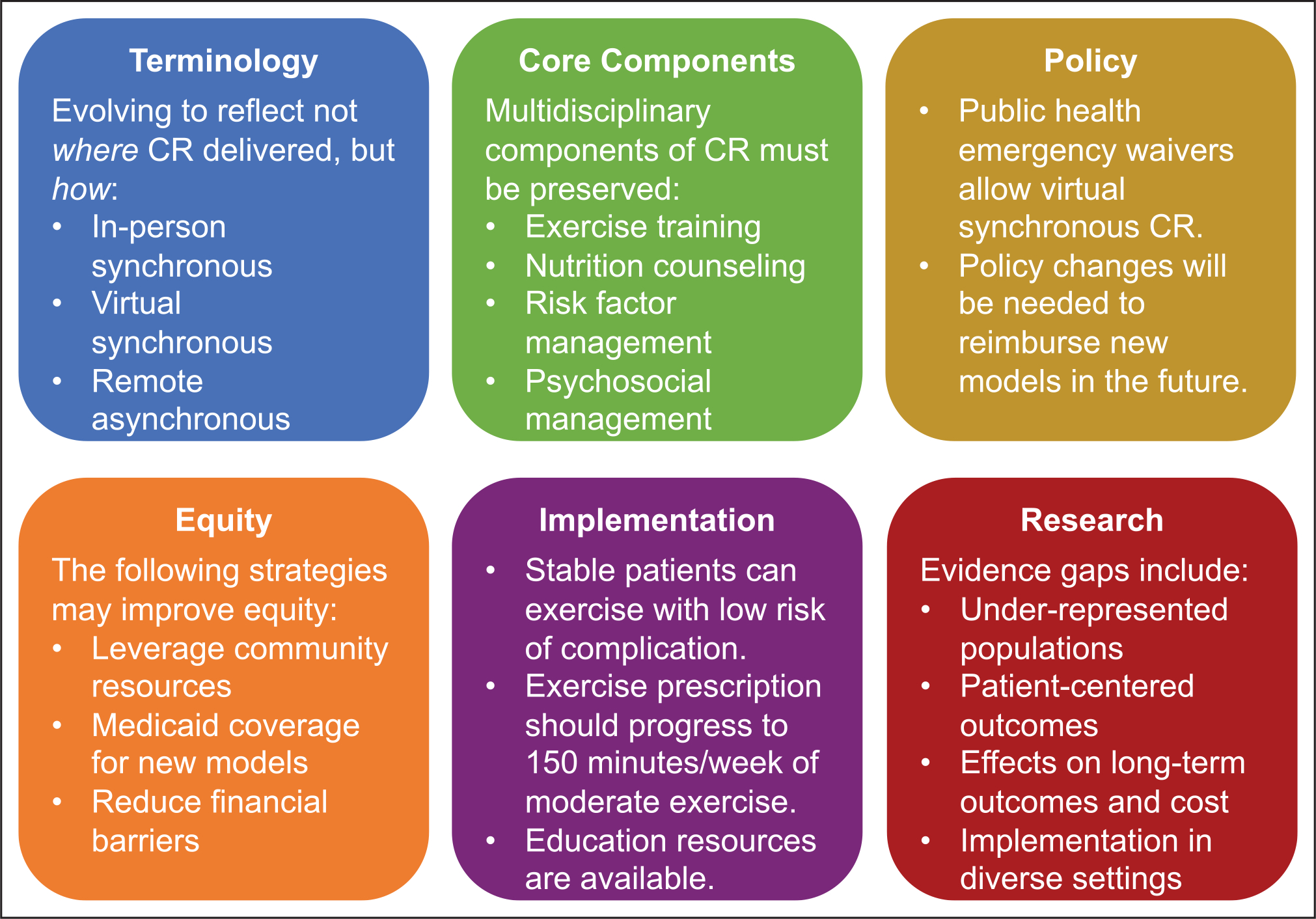
This article describes the October 2020 proceedings of the Million Hearts Cardiac Rehabilitation Think Tank: Accelerating New Care Models, convened with representatives from professional organizations, cardiac rehabilitation (CR) programs, academic institutions, federal agencies, payers, and patient representative groups. As CR delivery evolves, terminology is evolving to reflect not where activities occur (eg, center, home) but how CR is delivered: in-person synchronous, synchronous with real-time audiovisual communication (virtual), or asynchronous (remote). Patients and CR staff may interact through ≥1 delivery modes. Though new models may change how CR is delivered and who can access CR, new models should not change what is delivered-a multidisciplinary program addressing CR core components. During the coronavirus disease 2019 (COVID-19) public health emergency, Medicare issued waivers to allow virtual CR; it is unclear whether these waivers will become permanent policy post-public health emergency. Given CR underuse and disparities in delivery, new models must equitably address patient and health system contributors to disparities. Strategies for implementing new CR care models address safety, exercise prescription, monitoring, and education. The available evidence supports the efficacy and safety of new CR care models. Still, additional research should study diverse populations, impact on patient-centered outcomes, effect on long-term outcomes and health care utilization, and implementation in diverse settings. CR is evolving to include in-person synchronous, virtual, and remote modes of delivery; there is significant enthusiasm for implementing new care models and learning how new care models can broaden access to CR, improve patient outcomes, and address health inequities.
本文描述了 2020 年 10 月百万心脏心脏康复思想库的会议记录:加速新的护理模式,该会议召集了专业组织、心脏康复 (CR) 项目、学术机构、联邦机构、支付方和患者代表团体的代表。随着 CR 服务的发展,术语也在不断发展,以反映活动发生的地点(例如,中心、家庭),而是反映 CR 的提供方式:面对面同步、实时视听通讯的同步(虚拟)或异步(远程)。患者和 CR 工作人员可能通过≥1 种提供模式进行互动。尽管新模式可能会改变 CR 的提供方式和谁可以获得 CR,但新模式不应改变提供的内容——一个多学科的项目,解决 CR 的核心组成部分。在 2019 年冠状病毒病(COVID-19)公共卫生紧急情况下,医疗保险局发布了虚拟 CR 的豁免规定;尚不清楚这些豁免规定在公共卫生紧急情况后是否会成为永久政策。鉴于 CR 的使用率较低,以及在提供方面的差异,新模式必须公平地解决导致差异的患者和卫生系统的贡献者。实施新的 CR 护理模式的策略包括安全性、运动处方、监测和教育。现有证据支持新的 CR 护理模式的疗效和安全性。尽管如此,还需要更多的研究来研究不同人群、对以患者为中心的结果的影响、对长期结果和医疗保健利用的影响,以及在不同环境中的实施情况。CR 正在发展,包括面对面同步、虚拟和远程提供模式;人们对实施新的护理模式非常感兴趣,并希望了解新的护理模式如何扩大 CR 的可及性,改善患者的结果,并解决健康不公平问题。