Wu Shang-Gin, Liao Wei-Yu, Su Kang-Yi, Yu Sung-Liang, Huang Yen-Lin, Yu Chong-Jen, Chih-Hsin Yang James, Shih Jin-Yuan
Department of Internal Medicine, National Taiwan University Hospital, National Taiwan University, Taipei, Taiwan.
Department of Internal Medicine, National Taiwan University Cancer Center, National Taiwan University, Taipei, Taiwan.
JTO Clin Res Rep. 2020 Dec 26;2(2):100140. doi: 10.1016/j.jtocrr.2020.100140. eCollection 2021 Feb.
mutation is the most common driver oncogene present in patients with NSCLC. Recently, the precision medicine for patients with -mutated NSCLC has been under investigation, but the best treatment is still unknown. This study aimed to analyze the clinical characteristics, immune checkpoint inhibitor (ICI) response, and prognostic factors of patients with NSCLC with different mutation subtypes.
From 2005 to 2018, we collected nonsquamous NSCLC tissue samples for mutation analysis using direct Sanger sequencing or MassARRAY genotyping (Agena Bioscience, San Diego, CA) at the National Taiwan University Hospital. Clinical characteristics, ICI treatment effectiveness, time-to-tumor recurrence (TTR), and overall survival (OS) were analyzed using multivariate Cox models, to estimate adjusted hazard ratios (HRs).
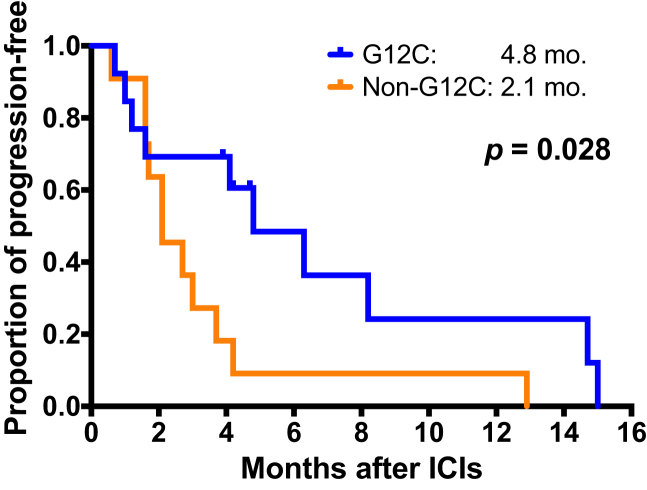
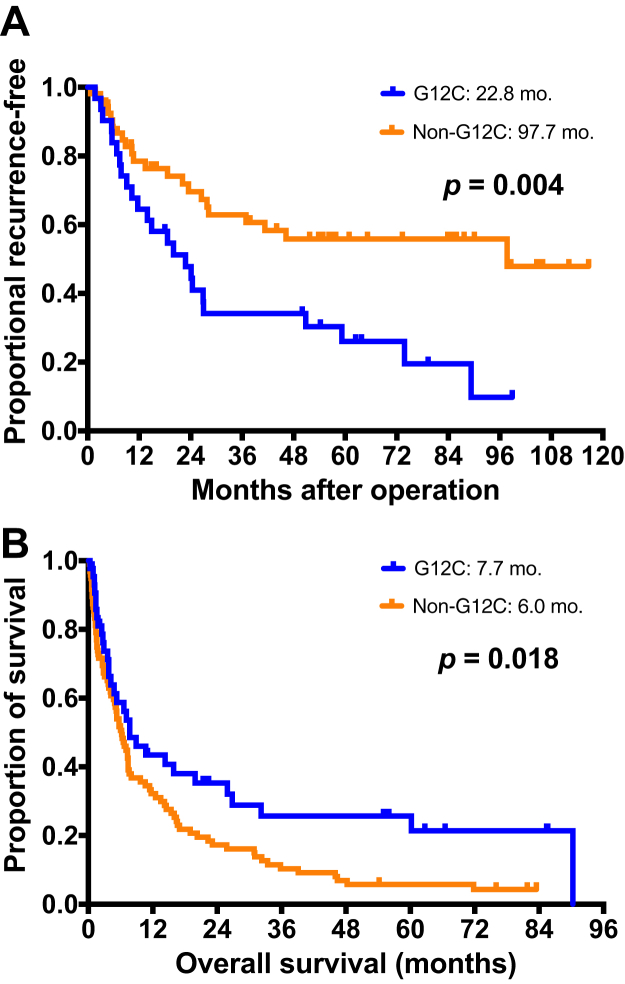
Among 5278 patients with nonsquamous NSCLC, 246 (4.7%) had mutations. The major mutation subtypes were G12C (32.9%), G12D (23.7%), and G12V (18.9%). Patients with -G12C had a higher proportion of male individuals ( = 0.018) and smokers ( < 0.001). Among the 25 patients treated with ICIs, patients with -G12C had a higher response rate (53.8% versus 8.3%, = 0.030) and longer progression-free survival (4.8 mo versus 2.1 mo, = 0.028) than those with -non-G12C. For the 85 patients with early-stage NSCLC, those with G12C had shorter TTR (22.8 mo) than those with -non-G12C (97.7 mo, = 0.004). For the 143 patients with advanced-stage NSCLC, there was a significant difference in OS between patients with -G12C and -non-G12C (7.7 mo versus 6.0 mo, = 0.018) and patients with -G12V had the shortest OS (5.2 mo). Multivariate analysis revealed association of shorter OS with -G12V (HR = 2.47, = 0.002), stage IV disease status (HR = 2.69, = 0.008), and NSCLC-not otherwise specified histology (HR = 3.12, = 0.002).
-G12C was associated with favorable ICI treatment effectiveness in patients with NSCLC. -G12C mutation was associated with shorter TTR in patients with early-stage NSCLC, and -G12V mutation was associated with shorter OS in patients with advanced-stage NSCLC when comparing with -G12C.
突变是NSCLC患者中最常见的驱动癌基因。最近,针对突变型NSCLC患者的精准医学研究一直在进行,但最佳治疗方案仍不明确。本研究旨在分析不同突变亚型的NSCLC患者的临床特征、免疫检查点抑制剂(ICI)反应及预后因素。
2005年至2018年,我们在台湾大学医院收集了非鳞状NSCLC组织样本,采用直接桑格测序或MassARRAY基因分型(Agena Bioscience,加利福尼亚州圣地亚哥)进行突变分析。使用多变量Cox模型分析临床特征、ICI治疗效果、肿瘤复发时间(TTR)和总生存期(OS),以估计调整后的风险比(HRs)。
在5278例非鳞状NSCLC患者中,246例(4.7%)存在突变。主要的突变亚型为G12C(32.9%)、G12D(23.7%)和G12V(18.9%)。G12C突变患者中男性个体(P = 0.018)和吸烟者比例更高(P < 0.001)。在25例接受ICI治疗的患者中,G12C突变患者的缓解率更高(53.8%对8.3%,P = 0.030),无进展生存期更长(4.8个月对2.1个月,P = 0.028)。对于85例早期NSCLC患者,G12C突变患者的TTR(22.8个月)短于非G12C突变患者(97.7个月,P = 0.004)。对于143例晚期NSCLC患者,G12C突变患者与非G12C突变患者的OS存在显著差异(7.7个月对6.0个月,P = 0.018),G12V突变患者的OS最短(5.2个月)。多变量分析显示,OS缩短与G12V突变(HR = 2.47,P = 0.002)、IV期疾病状态(HR = 2.69,P = 0.008)和非特指组织学类型的NSCLC(HR = 3.12,P = 0.002)相关。
G12C突变与NSCLC患者ICI治疗效果良好相关。与G12C突变相比,G12C突变与早期NSCLC患者的TTR缩短相关,G12V突变与晚期NSCLC患者的OS缩短相关。