Jendle Johan, Buompensiere M I, Holm A L, de Portu S, Malkin S J P, Cohen O
Institute of Medical Sciences, Campus USÖ, Örebro University, 701 82, Örebro, Sweden.
Medtronic International Trading Sàrl, Tolochenaz, Switzerland.
Diabetes Ther. 2021 Nov;12(11):2977-2991. doi: 10.1007/s13300-021-01157-0. Epub 2021 Oct 1.
Swedish National Diabetes Registry data show a correlation of improved glycemic control in people with type 1 diabetes (T1D) with increased use of diabetes technologies over the past 25 years. However, novel technologies are often associated with a high initial outlay. The aim of the present study was to evaluate the long-term cost-effectiveness of the advanced hybrid closed-loop (AHCL) MiniMed 780G system versus intermittently scanned continuous glucose monitoring (isCGM) plus self-injection of multiple daily insulin (MDI) or continuous subcutaneous insulin infusion (CSII) in people with T1D in Sweden.
Outcomes were projected over patients' lifetimes using the IQVIA CORE Diabetes Model (v9.0). Clinical data, including changes in glycated hemoglobin (HbA1c) and hypoglycemia rates, were sourced from observational studies and a randomized crossover trial. Modeled patients were assumed to receive the treatments for their lifetimes, with HbA1c kept constant following the application of treatment effects. Costs were accounted from a societal perspective and expressed in Swedish krona (SEK). Utilities and days off work estimates were taken from published sources.
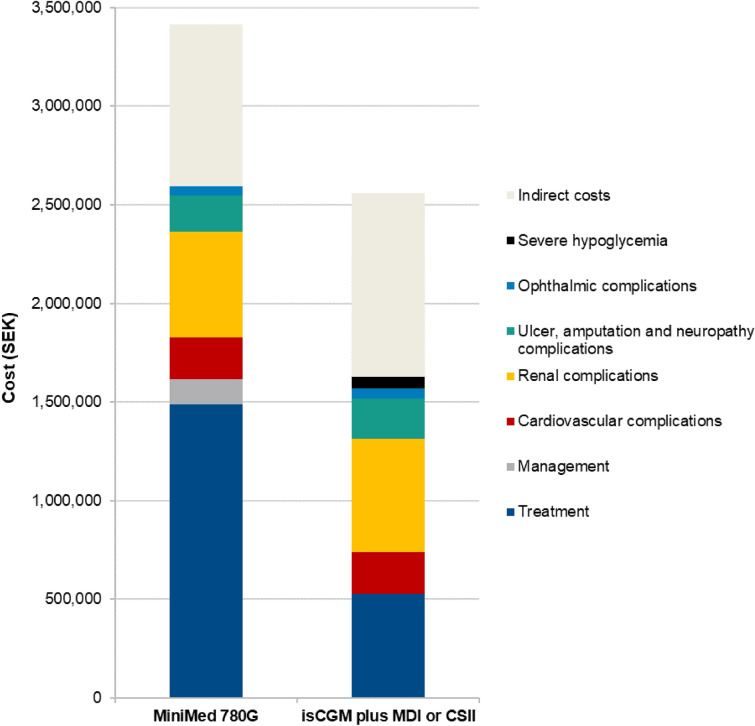
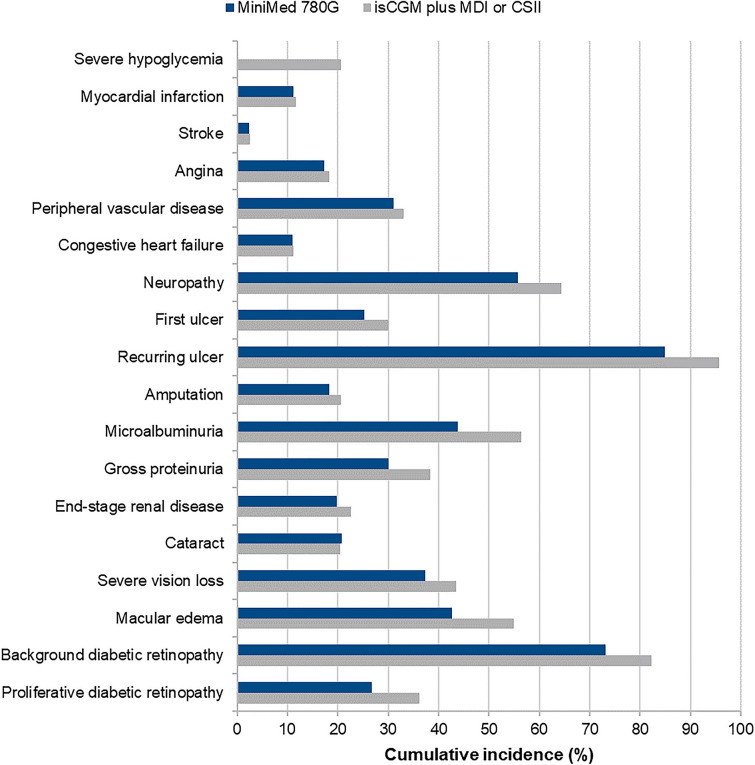
The MiniMed 780G system was associated with an improvement in life expectancy of 0.16 years and an improvement in quality-adjusted life expectancy of 1.95 quality-adjusted life years (QALYs) versus isCGM plus MDI or CSII. These clinical benefits were due to a reduced incidence and a delayed time to onset of diabetes-related complications. Combined costs were estimated to be SEK 727,408 (EUR 72,741) higher with MiniMed 780G, with treatment costs partially offset by direct cost savings from the avoidance of diabetes-related complications and indirect cost savings from the avoidance of lost workplace productivity. The MiniMed 780G system was associated with an incremental cost-effectiveness ratio of SEK 373,700 per QALY gained.
Based on a willingness-to-pay threshold of SEK 500,000 per QALY gained, the MiniMed 780G system was projected to be cost-effective versus isCGM plus MDI or CSII for the treatment of T1D in Sweden.
瑞典国家糖尿病登记处的数据显示,在过去25年里,1型糖尿病(T1D)患者血糖控制的改善与糖尿病技术使用的增加相关。然而,新技术往往伴随着较高的初始支出。本研究的目的是评估在瑞典,与间歇性扫描式动态血糖监测(isCGM)加每日多次胰岛素自我注射(MDI)或持续皮下胰岛素输注(CSII)相比,先进的混合闭环(AHCL)美敦力780G系统在T1D患者中的长期成本效益。
使用IQVIA CORE糖尿病模型(v9.0)预测患者一生的治疗结果。临床数据,包括糖化血红蛋白(HbA1c)的变化和低血糖发生率,来源于观察性研究和一项随机交叉试验。假定模型中的患者一生都接受这些治疗,在应用治疗效果后HbA1c保持不变。成本从社会角度计算,以瑞典克朗(SEK)表示。效用和误工天数估计值来自已发表的资料。
与isCGM加MDI或CSII相比,美敦力780G系统使预期寿命延长0.16年,质量调整生命预期延长1.95个质量调整生命年(QALY)。这些临床益处归因于糖尿病相关并发症的发生率降低和发病时间延迟。美敦力780G的总成本估计高出727,408瑞典克朗(72,741欧元),治疗成本部分被因避免糖尿病相关并发症而节省的直接成本以及因避免工作场所生产力损失而节省的间接成本所抵消。美敦力780G系统每获得一个QALY的增量成本效益比为373,700瑞典克朗。
基于每获得一个QALY支付意愿阈值为500,000瑞典克朗,预计在瑞典治疗T1D时,美敦力780G系统相对于isCGM加MDI或CSII具有成本效益。