Department of Epidemiology and Population Health, Stanford University School of Medicine, Stanford, CA, USA.
Division of General Internal Medicine and Primary Care, Department of Medicine, Brigham and Women's Hospital, Boston, MA, USA; Harvard Medical School, Boston, MA, USA.
Drug Alcohol Depend. 2021 Nov 1;228:109081. doi: 10.1016/j.drugalcdep.2021.109081. Epub 2021 Sep 24.
Effective, evidence-based treatments for opioid use disorder are not equally accessible to Americans. Recent studies have found urban/rural disparities in the driving times to the nearest opioid treatment providers. These disparities may be even worse than currently reported in the literature because patients may not be able to obtain appointments with their nearest provider. We examine the robustness of the opioid treatment infrastructure by estimating how driving times to treatment change as provider availability decreases.
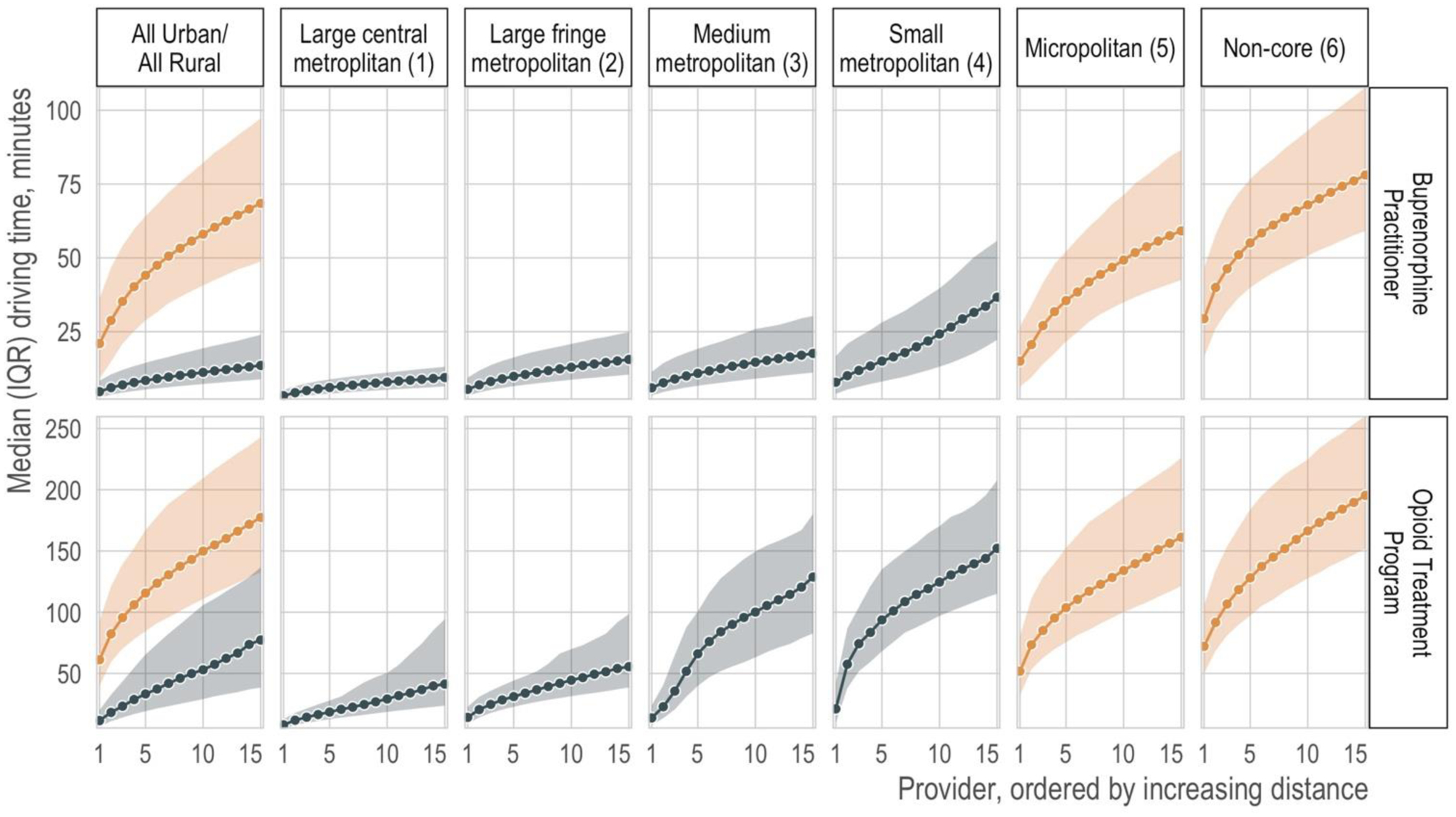
We used public data from the federal government to estimate the driving time from each census tract centroid to the nearest 15 treatment providers. We summarized the median and interquartile range of driving times to increasingly distant providers (i.e., nearest, second nearest, etc.), stratified by urban/rural classification.
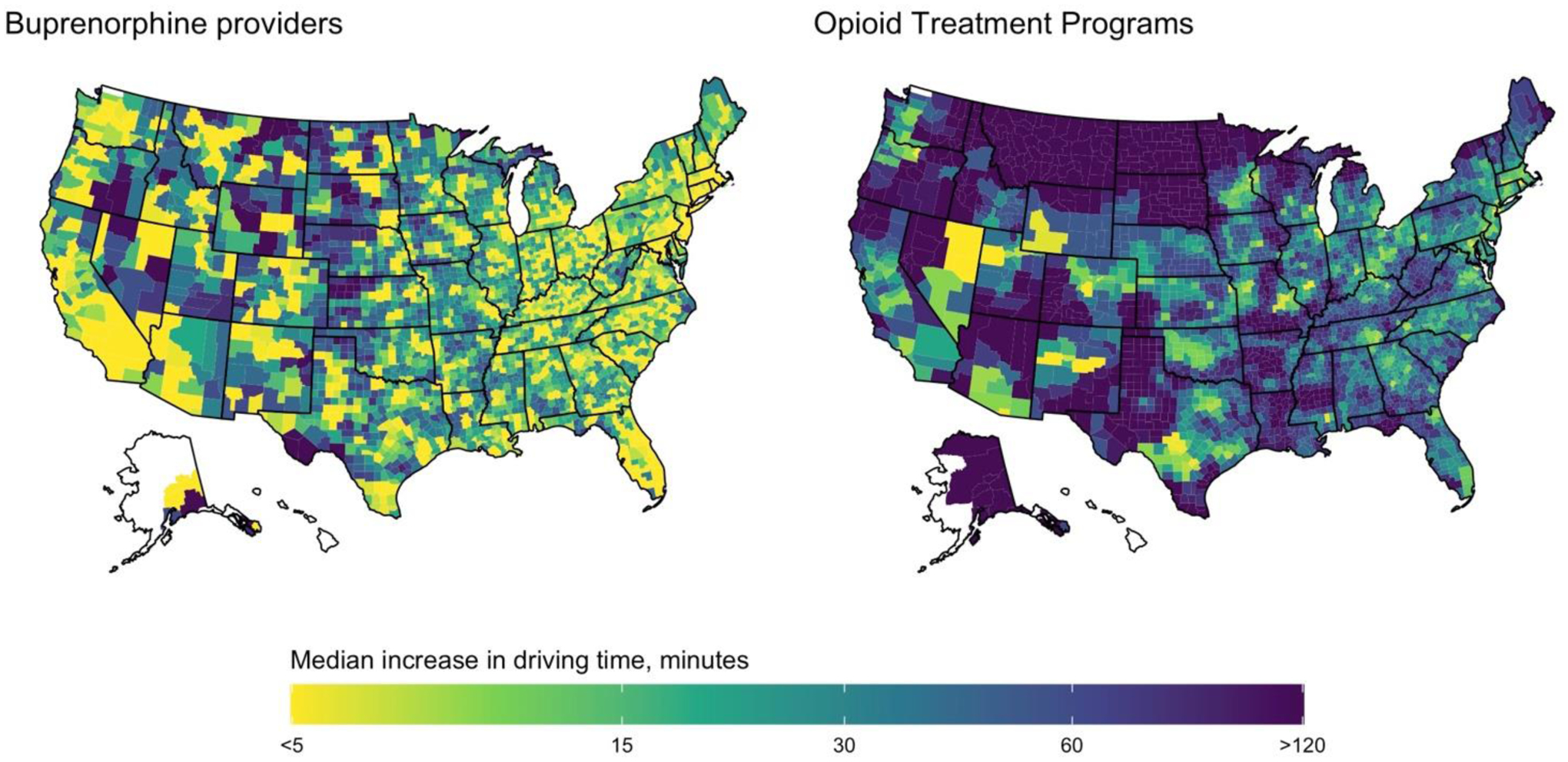
The median driving time to the nearest provider was greater in rural areas than urban areas for both opioid treatment programs (12 min vs 61 min) and buprenorphine-waivered prescribers (5 min vs 21 min). Importantly, driving times in rural areas increased more steeply as nearer providers became unavailable. For example, the increase in driving time between the nearest provider and the fifth nearest provider was much greater in rural areas than in urban areas for both buprenorphine-waivered prescribers (23 min vs 4 min) and for opioid treatment programs (54 min vs 22 min).
Access to treatment for opioid use disorder is more robust in urban areas compared with rural areas. This disparity must be eliminated if the opioid overdose crisis is to be resolved.
有效的、基于证据的阿片类药物使用障碍治疗方法在美国并非人人都能平等获得。最近的研究发现,在到达最近的阿片类药物治疗提供者的驾驶时间方面存在城乡差异。这些差异可能比目前文献中报道的更为严重,因为患者可能无法获得离他们最近的提供者的预约。我们通过估计随着提供者可用性的降低,治疗的驾驶时间如何变化来检查阿片类药物治疗基础设施的稳健性。
我们使用来自联邦政府的公共数据来估计从每个普查区质心到最近的 15 个治疗提供者的驾驶时间。我们按城乡分类总结了到越来越远的提供者(即最近、第二近等)的驾驶时间的中位数和四分位距。
在农村地区,到最近提供者的驾驶时间中位数大于城市地区,无论是在阿片类药物治疗计划(12 分钟对 61 分钟)还是在丁丙诺啡豁免处方者(5 分钟对 21 分钟)中都是如此。重要的是,在农村地区,随着更近的提供者变得不可用,驾驶时间增加得更陡峭。例如,对于丁丙诺啡豁免处方者(23 分钟对 4 分钟)和阿片类药物治疗计划(54 分钟对 22 分钟),在农村地区,从最近的提供者到第五近的提供者的驾驶时间增加幅度明显大于城市地区。
与农村地区相比,城市地区获得阿片类药物使用障碍治疗的途径更为稳健。如果要解决阿片类药物过量危机,就必须消除这种差异。