Centre of Molecular Inflammation Research, Norwegian University of Science and Technologygrid.5947.f, Trondheim, Norway.
Department of Clinical and Molecular Medicine, Faculty of Medicine and Health Sciences, Norwegian University of Science and Technologygrid.5947.f, Trondheim, Norway.
mBio. 2021 Oct 26;12(5):e0212121. doi: 10.1128/mBio.02121-21. Epub 2021 Oct 5.
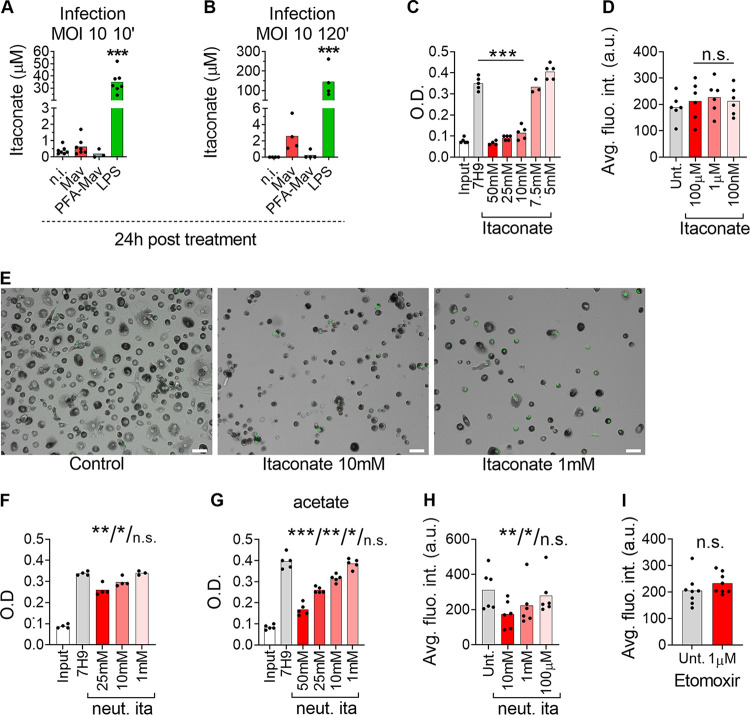
Macrophages sense and respond to pathogens by induction of antimicrobial and inflammatory programs to alert other immune cells and eliminate the infectious threat. We have previously identified the transcription factor IRF1 to be consistently activated in macrophages during Mycobacterium avium infection, but its precise role during infection is not clear. Here, we show that tumor necrosis factor alpha (TNF-α) and interleukin 6 (IL-6) autocrine/paracrine signaling contributes to controlling the intracellular growth of M. avium in human primary macrophages through activation of IRF1 nuclear translocation and expression of IRG1, a mitochondrial enzyme that produces the antimicrobial metabolite itaconate. Small interfering RNA (siRNA)-mediated knockdown of IRF1 or IRG1 increased the mycobacterial load, whereas exogenously provided itaconate was bacteriostatic at high concentrations. While the overall level of endogenous itaconate was low in M. avium-infected macrophages, the repositioning of mitochondria to M. avium phagosomes suggests a mechanism by which itaconate can be delivered directly to M. avium phagosomes in sufficient quantities to inhibit growth. Using mRNA hybridization, we further show that uninfected bystander cells actively contribute to the resolution of infection by producing IL-6 and TNF-α, which, via paracrine signaling, activate IRF1/IRG1 and strengthen the antimicrobial activity of infected macrophages. This mechanism contributes to the understanding of why patients on anti-inflammatory treatment, e.g., with tocilizumab or infliximab, can be more susceptible to mycobacterial disease. The prevalence of lung diseases caused by nontuberculous mycobacteria, such as Mycobacterium avium, is increasing in countries where tuberculosis is not endemic, most likely because of an aging population that is immunocompromised from underlying disease or immunosuppressive therapy. Our study contributes to the understanding of mycobacterial survival and killing in human macrophages and, more broadly, to the impact of immunometabolism during infection. We show evidence of an antimicrobial program in human primary macrophages where activation of the transcription factor IRF1 and expression of the mitochondrial enzyme IRG1 restrict the intracellular growth of M. avium, possibly by directed delivery of itaconate to M. avium phagosomes. The study also sheds light on why patients on immunosuppressive therapy are more susceptible to mycobacterial infections, since TNF-α and IL-6 contribute to driving the described antimycobacterial program.
巨噬细胞通过诱导抗菌和炎症程序来感知和应对病原体,以提醒其他免疫细胞并消除感染威胁。我们之前已经确定,转录因子 IRF1 在分枝杆菌感染的巨噬细胞中始终被激活,但它在感染过程中的精确作用尚不清楚。在这里,我们表明肿瘤坏死因子-α (TNF-α) 和白细胞介素 6 (IL-6) 自分泌/旁分泌信号通过激活 IRF1 核易位和表达线粒体酶 IRG1 来控制分枝杆菌在人原代巨噬细胞中的细胞内生长,IRG1 产生抗菌代谢物衣康酸。用小干扰 RNA (siRNA) 介导的 IRF1 或 IRG1 敲低增加了分枝杆菌负荷,而外源性提供的衣康酸在高浓度时具有抑菌作用。虽然分枝杆菌感染的巨噬细胞中内源性衣康酸的总体水平较低,但线粒体向分枝杆菌吞噬体的重定位表明了一种机制,通过该机制衣康酸可以直接递送至分枝杆菌吞噬体,以达到抑制生长的足够量。通过 mRNA 杂交,我们进一步表明,未感染的旁观者细胞通过产生白细胞介素 6 和肿瘤坏死因子-α 积极促进感染的解决,通过旁分泌信号,激活 IRF1/IRG1 并增强感染巨噬细胞的抗菌活性。该机制有助于理解为什么接受抗炎治疗(例如,使用托珠单抗或英夫利昔单抗)的患者更容易患分枝杆菌病。非结核分枝杆菌(如分枝杆菌)引起的肺部疾病的患病率在结核病非地方性国家正在增加,这很可能是由于人口老龄化,由于潜在疾病或免疫抑制治疗而使免疫系统受损。我们的研究有助于理解分枝杆菌在人原代巨噬细胞中的存活和杀伤,更广泛地说,有助于理解感染期间免疫代谢的影响。我们在人原代巨噬细胞中发现了一种抗菌程序的证据,其中转录因子 IRF1 的激活和线粒体酶 IRG1 的表达限制了分枝杆菌的细胞内生长,可能通过将衣康酸定向递送至分枝杆菌吞噬体来实现。该研究还揭示了为什么接受免疫抑制治疗的患者更容易感染分枝杆菌,因为 TNF-α 和 IL-6 有助于驱动所描述的抗分枝杆菌程序。