Instituto de Investigaciones Biomédicas en Retrovirus y SIDA. Facultad de Medicina. UBA-CONICET. Paraguay 2155, C1121ABG CABA, Argentina.
Departamento de Medicina, Hospital General de Niños Pedro de Elizalde. Av. Montes de Oca 40, C1270 CABA, Argentina.
EBioMedicine. 2021 Oct;72:103615. doi: 10.1016/j.ebiom.2021.103615. Epub 2021 Oct 11.
Most children and youth develop mild or asymptomatic disease during severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection. However, a very small number of patients suffer severe Coronavirus induced disease 2019 (COVID-19). The reasons underlying these different outcomes remain unknown.
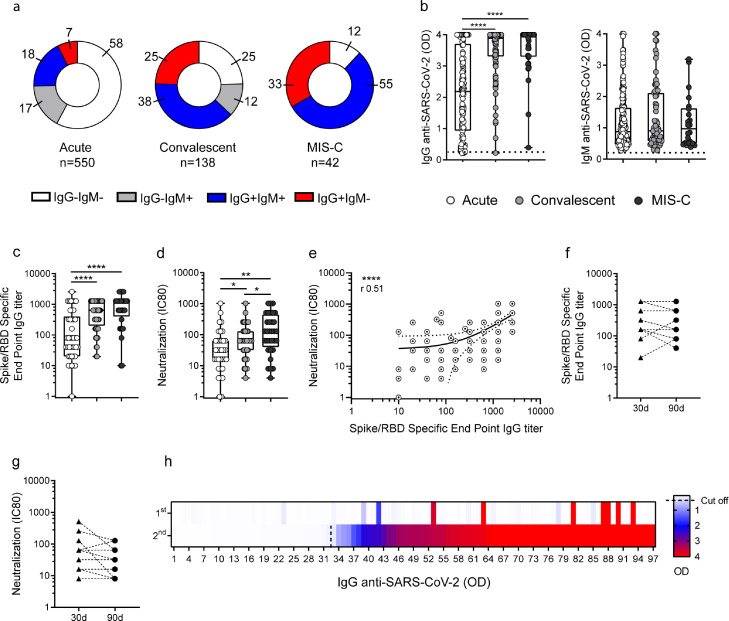
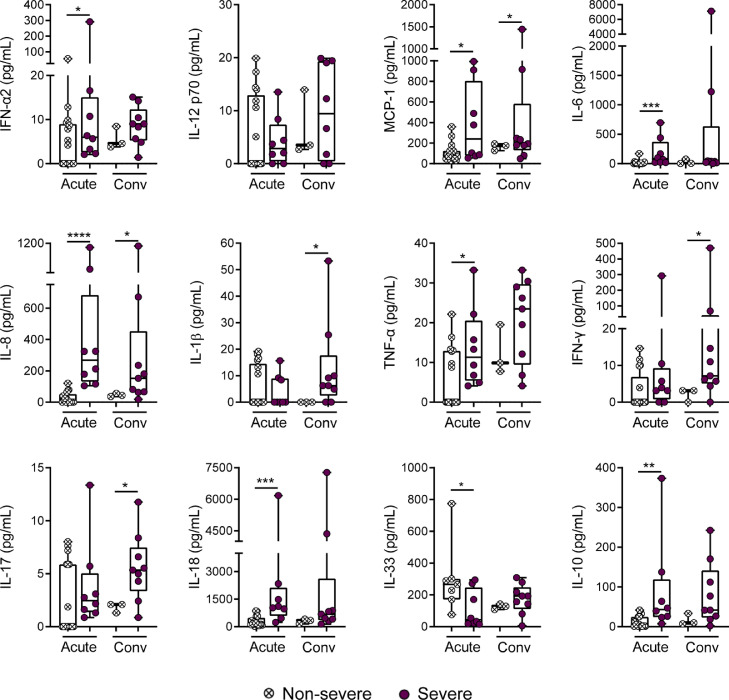
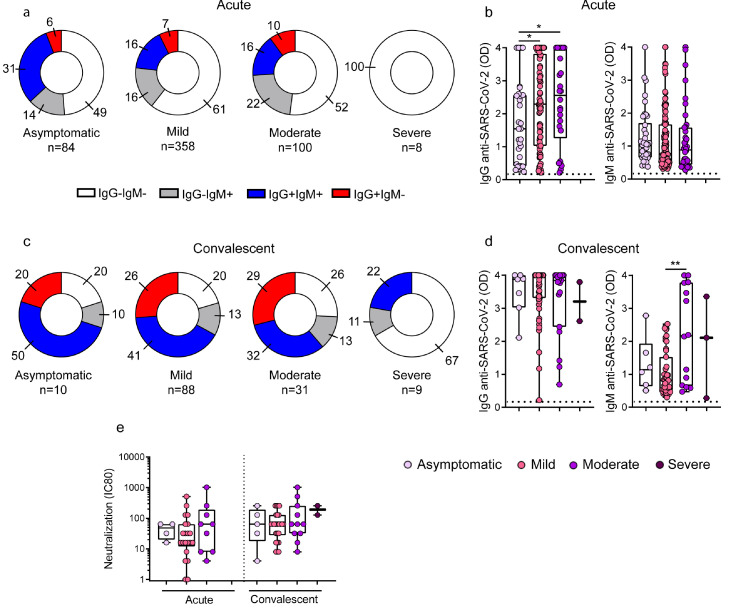
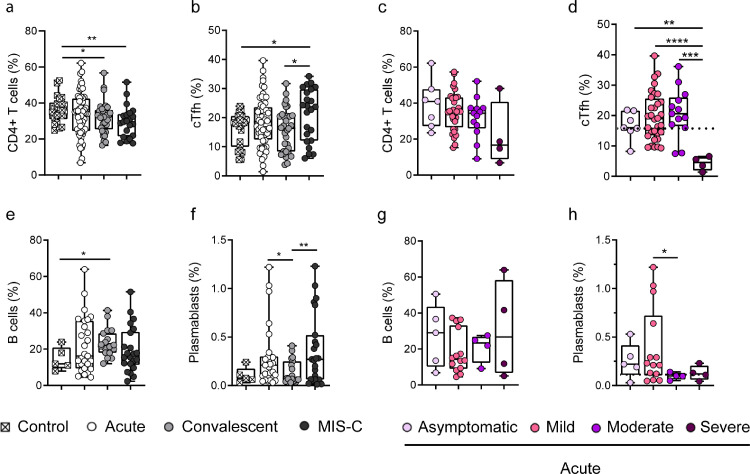
We analyzed three different cohorts: children with acute infection (n=550), convalescent children (n=138), and MIS-C (multisystem inflammatory syndrome in children, n=42). IgG and IgM antibodies to the spike protein of SARS-CoV-2, serum-neutralizing activity, plasma cytokine levels, and the frequency of circulating Follicular T helper cells (cTfh) and plasmablasts were analyzed by conventional methods.
Fifty-eight percent of the children in the acute phase of infection had no detectable antibodies at the time of sampling while a seronegative status was found in 25% and 12% of convalescent and MIS-C children, respectively. When children in the acute phase of the infection were stratified according disease severity, we found that contrasting with the response of children with asymptomatic, mild and moderate disease, children with severe COVID-19 did not develop any detectable response. A defective antibody response was also observed in the convalescent cohort for children with severe disease at the time of admission. This poor antibody response was associated to both, a low frequency of cTfh and a high plasma concentration of inflammatory cytokines.
A weak and delayed kinetic of antibody response to SARS-CoV-2 together with a systemic pro-inflammatory profile characterize pediatric severe COVID-19. Because comorbidities are highly prevalent in children with severe COVID-19, further studies are needed to clarify their contribution in the weak antibody response observed in severe disease.
National Agency for Scientific and Technological Promotion from Argentina (IP-COVID-19-0277 and PMO-BID-PICT2018-2548).
大多数儿童和青少年在严重急性呼吸综合征冠状病毒 2(SARS-CoV-2)感染期间会出现轻度或无症状疾病。然而,极少数患者患有严重的 2019 年冠状病毒病(COVID-19)。这些不同结果的原因尚不清楚。
我们分析了三个不同的队列:急性感染的儿童(n=550)、恢复期儿童(n=138)和 MIS-C(儿童多系统炎症综合征,n=42)。使用常规方法分析了 SARS-CoV-2 刺突蛋白的 IgG 和 IgM 抗体、血清中和活性、血浆细胞因子水平以及循环滤泡辅助 T 细胞(cTfh)和浆母细胞的频率。
在感染急性期,58%的儿童在采样时未检测到抗体,而恢复期和 MIS-C 儿童的血清阴性率分别为 25%和 12%。当根据疾病严重程度对感染急性期的儿童进行分层时,我们发现与无症状、轻度和中度疾病儿童的反应相反,严重 COVID-19 儿童没有产生任何可检测到的反应。在入院时患有严重疾病的恢复期儿童中,也观察到抗体反应缺陷。这种不良的抗体反应与 cTfh 的低频率和炎症细胞因子的高血浆浓度有关。
对 SARS-CoV-2 的弱而延迟的抗体反应动力学以及全身促炎特征是儿科严重 COVID-19 的特征。由于严重 COVID-19 儿童的合并症非常普遍,因此需要进一步研究以阐明它们在严重疾病中观察到的弱抗体反应中的贡献。
阿根廷国家科学技术促进局(IP-COVID-19-0277 和 PMO-BID-PICT2018-2548)。