Center for Cancer and Immunology Research, Children's National Hospital, Washington, DC, United States.
Division of Critical Care Medicine, Children's National Hospital, Washington, DC, United States.
Front Immunol. 2022 Jan 18;12:793197. doi: 10.3389/fimmu.2021.793197. eCollection 2021.
Despite similar rates of infection, adults and children have markedly different morbidity and mortality related to severe acute respiratory syndrome coronavirus-2 (SARS-CoV-2). Compared to adults, children have infrequent severe manifestations of acute infection but are uniquely at risk for the rare and often severe Multisystem Inflammatory Syndrome in Children (MIS-C) following infection. We hypothesized that these differences in presentation are related to differences in the magnitude and/or antigen specificity of SARS-CoV-2-specific T cell (CST) responses between adults and children. We therefore set out to measure the CST response in convalescent adults versus children with and without MIS-C following SARS-CoV-2 infection.
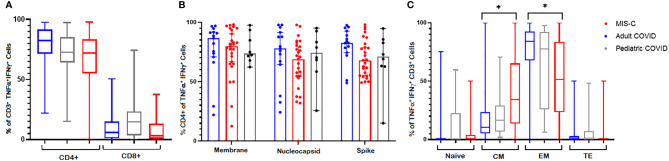
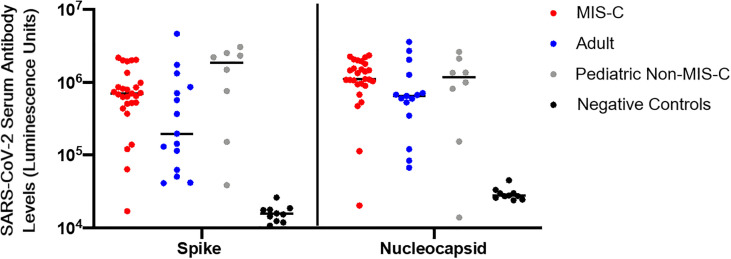
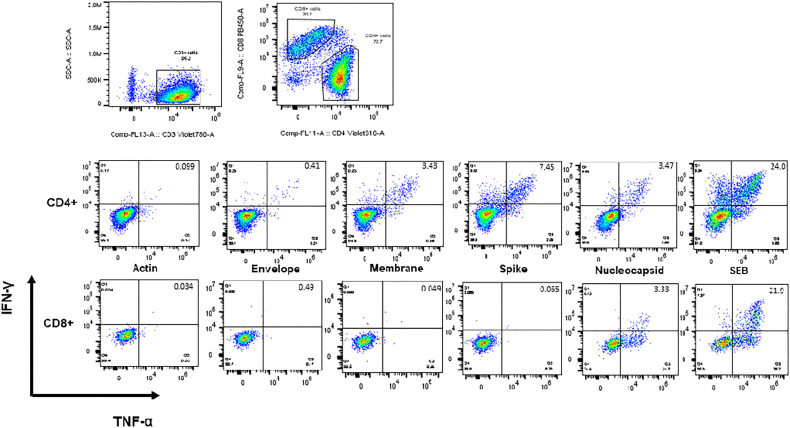
CSTs were expanded from blood collected from convalescent children and adults post SARS-CoV-2 infection and evaluated by intracellular flow cytometry, surface markers, and cytokine production following stimulation with SARS-CoV-2-specific peptides. Presence of serum/plasma antibody to spike and nucleocapsid was measured using the luciferase immunoprecipitation systems (LIPS) assay.
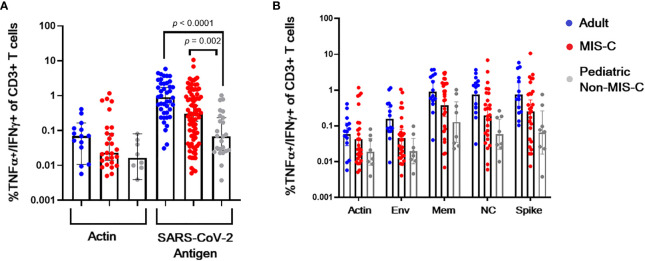
Twenty-six of 27 MIS-C patients, 7 of 8 non-MIS-C convalescent children, and 13 of 14 adults were seropositive for spike and nucleocapsid antibody. CST responses in MIS-C patients were significantly higher than children with uncomplicated SARS-CoV-2 infection, but weaker than CST responses in convalescent adults.
Age-related differences in the magnitude of CST responses suggest differing post-infectious immunity to SARS-CoV-2 in children compared to adults post uncomplicated infection. Children with MIS-C have CST responses that are stronger than children with uncomplicated SARS-CoV-2 infection and weaker than convalescent adults, despite near uniform seropositivity.
尽管成年人和儿童的感染率相似,但与严重急性呼吸综合征冠状病毒 2 型(SARS-CoV-2)相关的发病率和死亡率却有明显的不同。与成年人相比,儿童急性感染的严重表现较少,但在感染后,他们独特地面临罕见且通常严重的儿童多系统炎症综合征(MIS-C)的风险。我们假设,这些临床表现的差异与成人和儿童之间 SARS-CoV-2 特异性 T 细胞(CST)反应的幅度和/或抗原特异性的差异有关。因此,我们着手测量了 SARS-CoV-2 感染后康复的成人与无 MIS-C 和有 MIS-C 的儿童的 CST 反应。
从 SARS-CoV-2 感染后康复的儿童和成人的血液中扩增 CST,并通过细胞内流式细胞术、表面标志物和刺激后细胞因子的产生进行评估,使用 SARS-CoV-2 特异性肽进行刺激。使用荧光素酶免疫沉淀系统(LIPS)测定法测量血清/血浆中针对刺突和核衣壳的抗体。
27 例 MIS-C 患者中的 26 例、8 例非 MIS-C 恢复期儿童中的 7 例和 14 例成人中的 13 例对刺突和核衣壳抗体呈血清阳性。MIS-C 患者的 CST 反应明显高于无并发症 SARS-CoV-2 感染的儿童,但比康复的成年人的 CST 反应弱。
CST 反应幅度的年龄相关差异表明,与无并发症感染后的成年人相比,儿童在感染 SARS-CoV-2 后的免疫反应不同。患有 MIS-C 的儿童的 CST 反应强于无并发症 SARS-CoV-2 感染的儿童,但弱于康复的成年人,尽管血清阳性率几乎相同。