Univ. Lille, Inserm, CHU Lille, U1172 - LilNCog - Lille Neuroscience & Cognition, Lille, France.
Department of Neuroradiology, Roger Salengro Hospital, CHU Lille, University of Lille, Lille, France.
Eur Stroke J. 2023 Mar;8(1):199-207. doi: 10.1177/23969873221140649. Epub 2022 Dec 1.
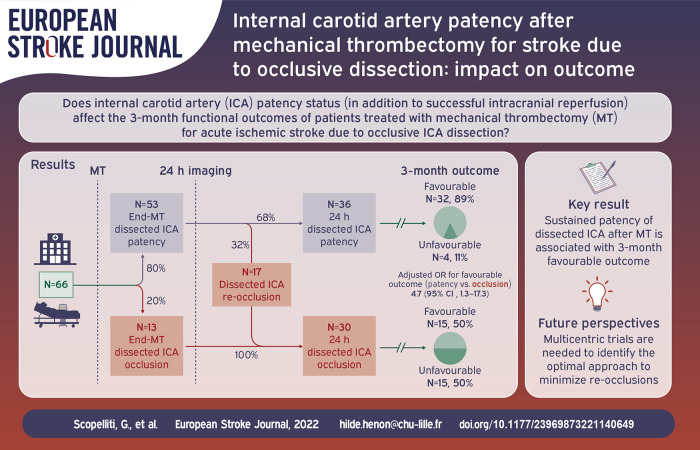
Internal carotid artery dissection (ICAD) is a rare cause of acute ischemic stroke with large vessel occlusion (AIS-LVO). We aimed investigating the impact on outcome of internal carotid artery (ICA) patency after mechanical thrombectomy (MT) for AIS-LVO due to occlusive ICAD.
We included consecutive patients with AIS-LVO due to occlusive ICAD treated with MT from January 2015 to December 2020 in three European stroke centers. We excluded patients with unsuccessful intracranial reperfusion after MT (modified Thrombolysis in Cerebral Infarction (mTICI) score < 2b). We compared 3-month favorable clinical outcome rate, defined as a modified Rankin scale (mRS) score ⩽2, according to ICA status (patency vs occlusion) at the end of MT and at 24-h follow-up imaging, using univariate and multivariable models.
Among 70 included patients, ICA was patent in 54/70 (77%) at the end of MT, and in 36/66 (54.5%) patients with 24-h follow-up imaging. Among patients with ICA patency at the end of MT, 32% presented ICA occlusion at 24-h control imaging. Favorable 3-month outcome occurred in 41/54 (76%) patients with ICA patency post-MT and in 9/16 (56%) patients with occluded ICA post-MT ( = 0.21). Rates of favorable outcome were significantly higher in patients with 24-h ICA patency compared to patients with 24-h ICA occlusion (32/36 [89%] vs 15/30 [50%]), with an adjusted odds ratio of 4.67 (95% CI: 1.26-17.25).
Obtaining sustained (24-h) ICA patency after MT could be a therapeutic target for improving functional outcome in patients with AIS-LVO due to ICAD.
颈内动脉夹层(ICAD)是大血管闭塞性急性缺血性卒中(AIS-LVO)的罕见病因。我们旨在研究机械血栓切除术(MT)治疗闭塞性颈内动脉夹层(ICAD)所致 AIS-LVO 后颈内动脉(ICA)通畅对结局的影响。
我们纳入了 2015 年 1 月至 2020 年 12 月在三个欧洲卒中中心接受 MT 治疗的、由闭塞性 ICAD 引起的 AIS-LVO 连续患者。我们排除了 MT 后颅内再通不成功的患者(改良脑梗死溶栓(mTICI)评分 < 2b)。我们使用单变量和多变量模型,根据 MT 结束时和 24 小时随访成像时 ICA 状态(通畅 vs 闭塞)比较 3 个月时的良好临床转归率,定义为改良 Rankin 量表(mRS)评分≤2。
在 70 例纳入患者中,MT 结束时 54/70(77%)的 ICA 通畅,66 例中有 36 例(54.5%)在 24 小时随访成像时有 ICA 通畅。在 MT 结束时 ICA 通畅的患者中,32%在 24 小时对照成像时出现 ICA 闭塞。MT 后 ICA 通畅的患者中有 41/54(76%)3 个月预后良好,MT 后 ICA 闭塞的患者中有 9/16(56%)预后良好( = 0.21)。与 24 小时 ICA 闭塞的患者相比,24 小时 ICA 通畅的患者预后良好的比例显著更高(32/36 [89%] vs 15/30 [50%]),校正比值比为 4.67(95%CI:1.26-17.25)。
MT 后获得持续(24 小时)ICA 通畅可能是改善 ICAD 引起的 AIS-LVO 患者功能结局的治疗靶点。