Liverpool Centre for Cardiovascular Science, University of Liverpool and Liverpool Heart & Chest Hospital, Liverpool, UK.
Geriatric Unit, IRCCS Istituti Clinici Scientifici Maugeri, Milan, Italy.
BMC Med. 2021 Oct 20;19(1):256. doi: 10.1186/s12916-021-02120-3.
Epidemiological studies in atrial fibrillation (AF) illustrate that clinical complexity increase the risk of major adverse outcomes. We aimed to describe European AF patients' clinical phenotypes and analyse the differential clinical course.
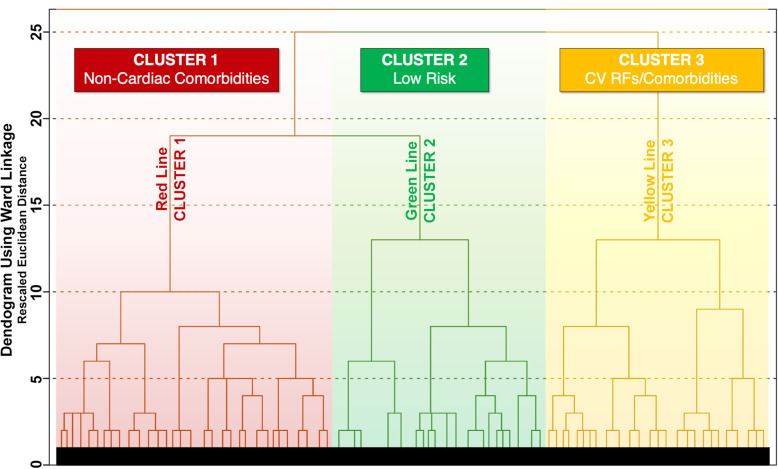
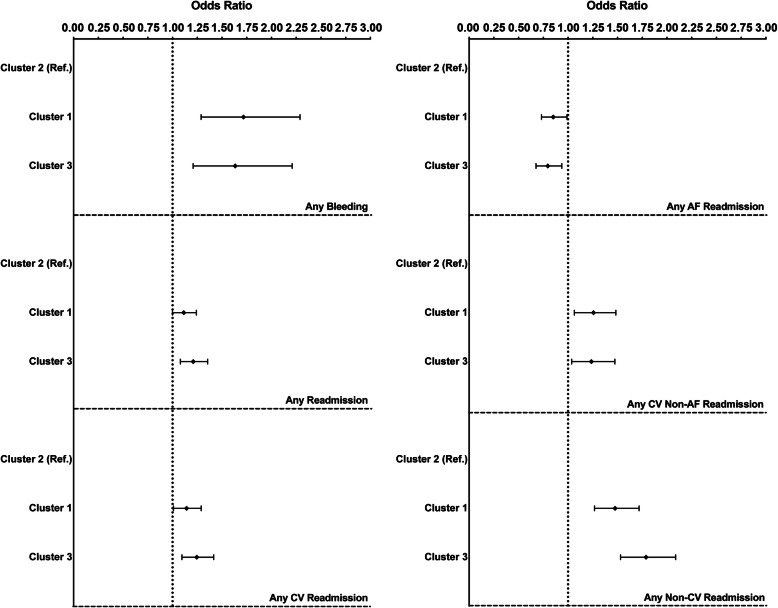
We performed a hierarchical cluster analysis based on Ward's Method and Squared Euclidean Distance using 22 clinical binary variables, identifying the optimal number of clusters. We investigated differences in clinical management, use of healthcare resources and outcomes in a cohort of European AF patients from a Europe-wide observational registry.
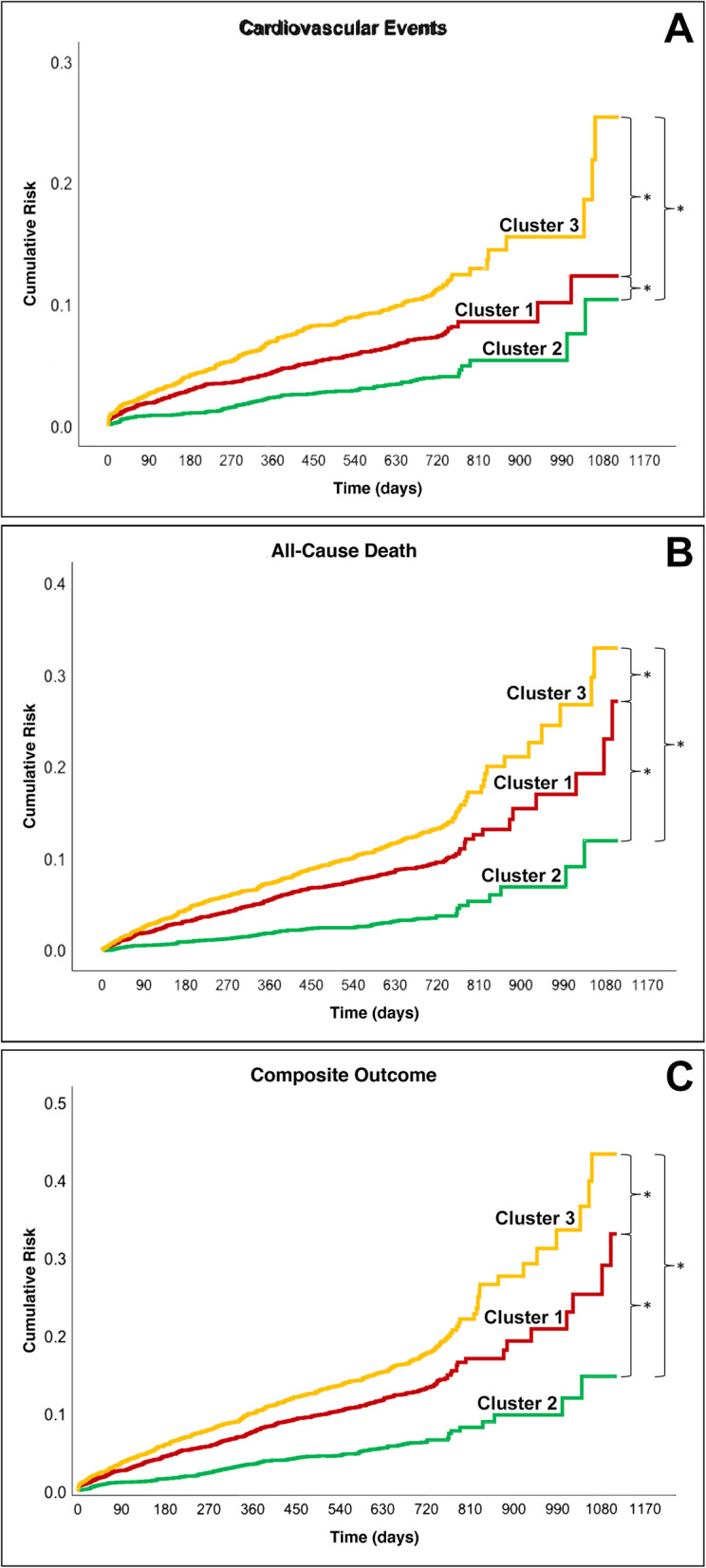
A total of 9363 were available for this analysis. We identified three clusters: Cluster 1 (n = 3634; 38.8%) characterized by older patients and prevalent non-cardiac comorbidities; Cluster 2 (n = 2774; 29.6%) characterized by younger patients with low prevalence of comorbidities; Cluster 3 (n = 2955;31.6%) characterized by patients' prevalent cardiovascular risk factors/comorbidities. Over a mean follow-up of 22.5 months, Cluster 3 had the highest rate of cardiovascular events, all-cause death, and the composite outcome (combining the previous two) compared to Cluster 1 and Cluster 2 (all P < .001). An adjusted Cox regression showed that compared to Cluster 2, Cluster 3 (hazard ratio (HR) 2.87, 95% confidence interval (CI) 2.27-3.62; HR 3.42, 95%CI 2.72-4.31; HR 2.79, 95%CI 2.32-3.35), and Cluster 1 (HR 1.88, 95%CI 1.48-2.38; HR 2.50, 95%CI 1.98-3.15; HR 2.09, 95%CI 1.74-2.51) reported a higher risk for the three outcomes respectively.
In European AF patients, three main clusters were identified, differentiated by differential presence of comorbidities. Both non-cardiac and cardiac comorbidities clusters were found to be associated with an increased risk of major adverse outcomes.
房颤(AF)的流行病学研究表明,临床复杂性增加了主要不良结局的风险。我们旨在描述欧洲 AF 患者的临床表型,并分析其不同的临床过程。
我们使用 22 个临床二分类变量,基于 Ward 法和平方欧几里得距离进行层次聚类分析,确定最佳聚类数。我们对来自欧洲范围内观察性注册的欧洲 AF 患者队列的临床管理、医疗资源使用和结局差异进行了研究。
共 9363 例患者可用于本分析。我们发现了三个聚类:聚类 1(n=3634;38.8%),特征为老年患者和常见的非心脏合并症;聚类 2(n=2774;29.6%),特征为年轻患者,合并症患病率低;聚类 3(n=2955;31.6%),特征为患者常见的心血管危险因素/合并症。在平均 22.5 个月的随访中,与聚类 1 和聚类 2 相比,聚类 3 的心血管事件、全因死亡和复合结局(前两者的组合)发生率最高(均 P<0.001)。调整后的 Cox 回归显示,与聚类 2 相比,聚类 3(风险比(HR)2.87,95%置信区间(CI)2.27-3.62;HR 3.42,95%CI 2.72-4.31;HR 2.79,95%CI 2.32-3.35)和聚类 1(HR 1.88,95%CI 1.48-2.38;HR 2.50,95%CI 1.98-3.15;HR 2.09,95%CI 1.74-2.51)的三种结局风险均更高。
在欧洲 AF 患者中,确定了三个主要聚类,其差异在于合并症的不同存在。非心脏和心脏合并症聚类均与主要不良结局风险增加相关。