De Giacomo Anthony F, Lu Young, Suh Dong Hun, McGarry Michelle H, Banffy Michael, Lee Thay Q
Southern California Permanente Medical Group, Woodland Hills, California, USA.
University of California, Irvine, Orange, California, USA.
Orthop J Sports Med. 2021 Oct 14;9(10):23259671211040098. doi: 10.1177/23259671211040098. eCollection 2021 Oct.
In hip arthroscopy, the best capsular closure technique to prevent microinstability in some patients while preventing overconstraints in other patients has yet to be determined.
To evaluate the biomechanical effects of capsular repair, capsular shift, and combination capsular shift and capsular plication for closure of the hip capsule.
Controlled laboratory study.
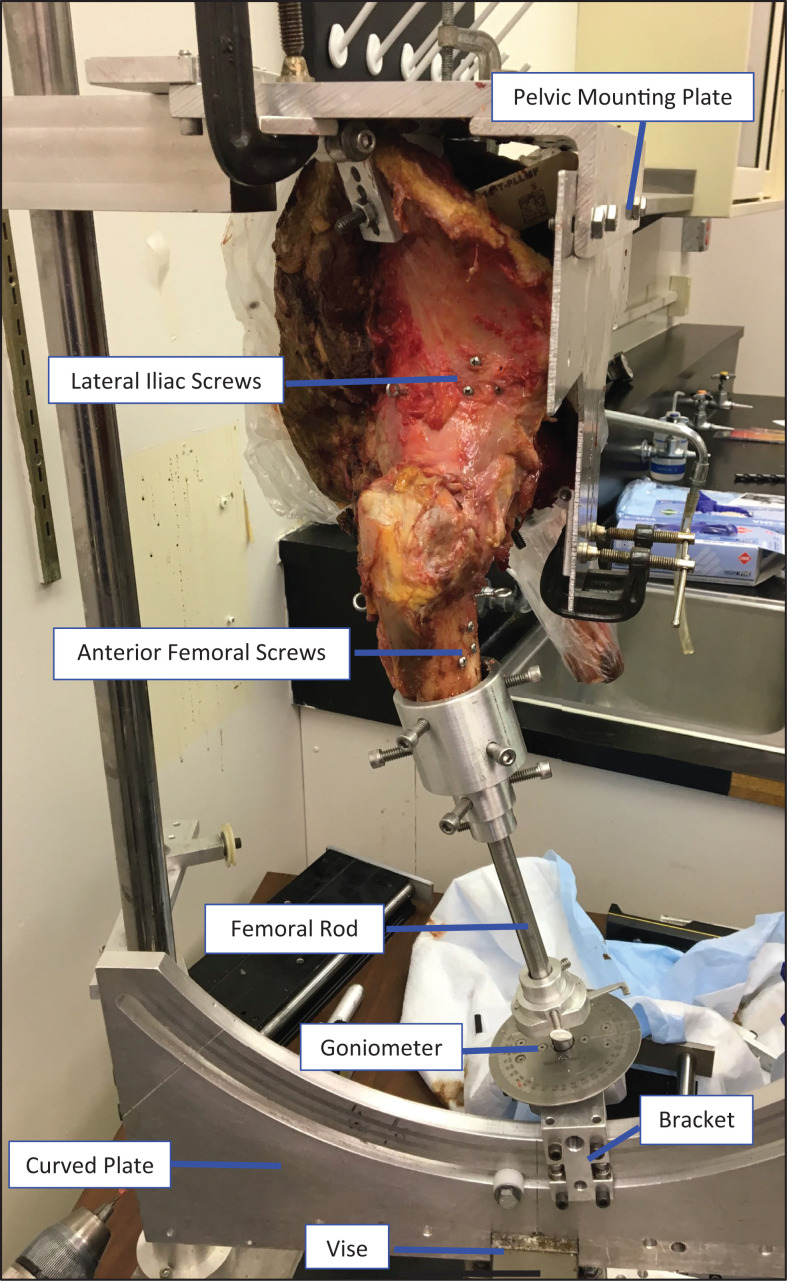
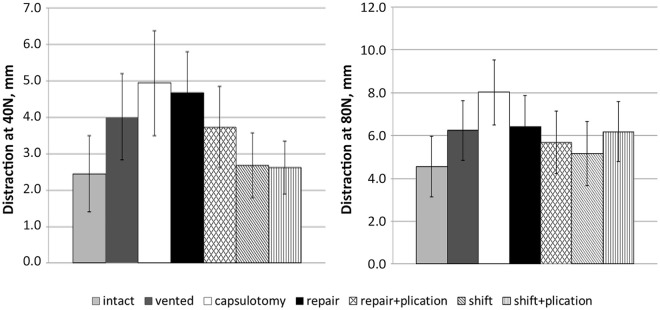
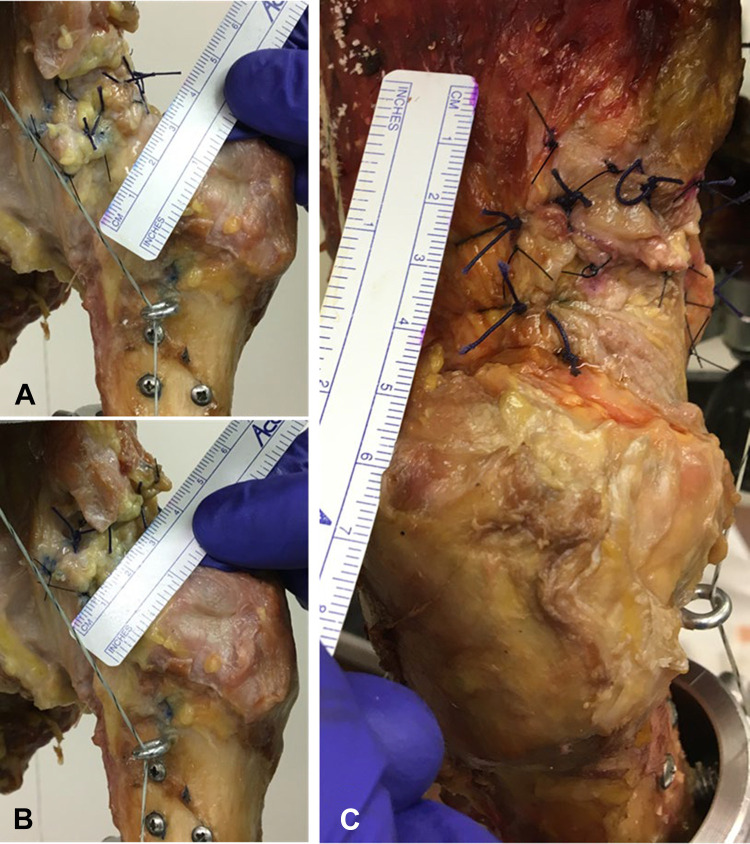
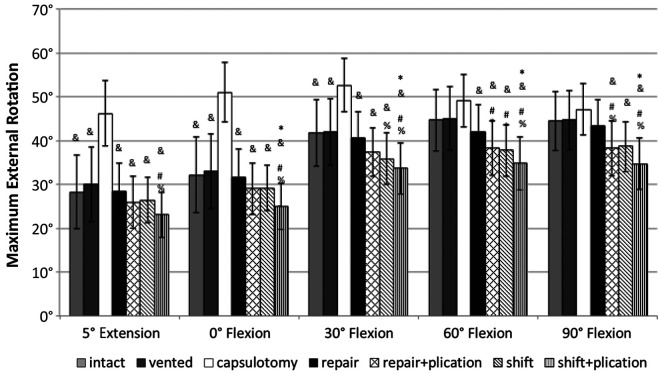
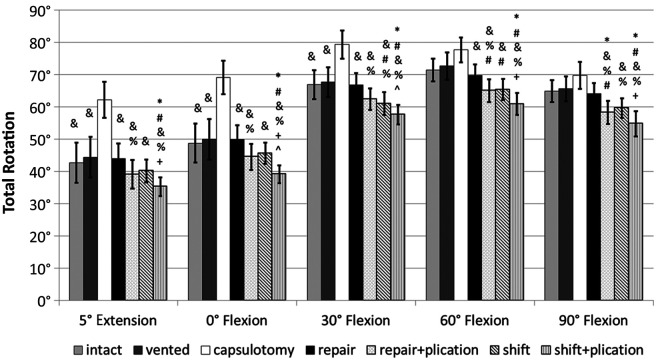
Eight cadaveric hips (4 male and 4 female hips; mean age, 55.7 years) were evaluated in 7 conditions: intact, vented, capsulotomy, side-to-side repair, side-to-side repair with capsular plication (interval closure between iliofemoral and ischiofemoral ligaments), capsular shift repair, and capsular shift repair with plication. Measurements, via a 360° goniometer, included internal and external rotation with 1.5 N·m of torque at 5° of extension and 0°, 30°, 60°, and 90° of flexion. In addition, the degree of maximum extension with 5 N·m of torque and the amount of femoral distraction with 40 N and 80 N of force were obtained. Repeated-measures analysis of variance and Tukey post hoc analyses were used to analyze differences between capsular conditions.
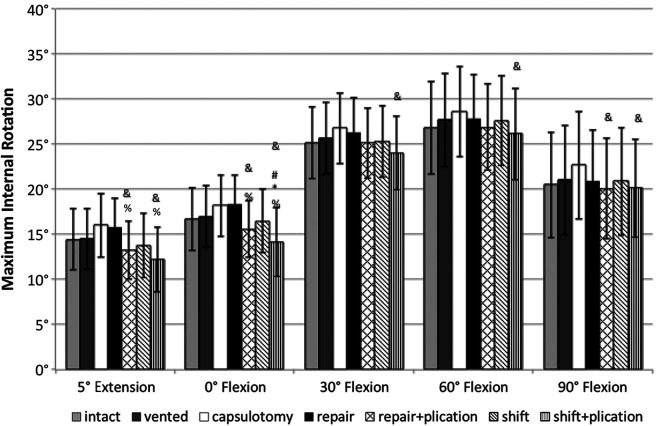
At lower hip positions (5° of extension, 0° and 30° of flexion), there was a significant increase in external rotation and total rotation after capsulotomy versus the intact state ( < .05). At all hip flexion angles, there was a significant increase in external rotation, internal rotation, and total rotation as well as a significant increase in maximum extension after capsulotomy versus capsular shift with plication ( < .05 for all). At all flexion angles, both capsular closure with side-to-side repair (with or without plication) and capsular shift without capsular plication were able to restore rotation, with no significant differences compared with the intact capsule ( > .05). Among repair constructs, there were significant differences in range of motion between side-to-side repair and combined capsular shift with plication ( < .05).
At all positions, significantly increased rotational motion was seen after capsulotomy. Capsular closure was able to restore rotation similar to an intact capsule. Combined capsular shift and plication may provide more restrained rotation for conditions of hip microinstability but may overconstrain hips without laxity.
More advanced closure techniques or a combination of techniques may be needed for patients with hip laxity and microinstability. At the same time, simple repair may suffice for patients without these conditions.
在髋关节镜检查中,尚未确定哪种最佳的关节囊闭合技术既能防止某些患者出现微不稳定,又能防止其他患者出现过度限制。
评估关节囊修复、关节囊移位以及关节囊移位与关节囊折叠联合应用对髋关节囊闭合的生物力学影响。
对照实验室研究。
对8具尸体髋关节(4具男性和4具女性髋关节;平均年龄55.7岁)在7种情况下进行评估:完整状态、打孔、关节囊切开、端端修复、端端修复并关节囊折叠(髂股韧带和坐骨股韧带之间的间隔闭合)、关节囊移位修复以及关节囊移位修复并折叠。通过360°测角仪进行测量,包括在伸展5°以及屈曲0°、30°、60°和90°时施加1.5 N·m扭矩下的内旋和外旋。此外,还获得了施加5 N·m扭矩时的最大伸展程度以及施加40 N和80 N力时的股骨牵开量。采用重复测量方差分析和Tukey事后分析来分析关节囊不同状态之间的差异。
在髋关节较低位置(伸展5°、屈曲0°和30°),与完整状态相比,关节囊切开后外旋和总旋转显著增加(P <.05)。在所有髋关节屈曲角度,与关节囊移位并折叠相比,关节囊切开后外旋、内旋和总旋转显著增加,最大伸展也显著增加(均P <.05)。在所有屈曲角度,端端修复(有或无折叠)的关节囊闭合以及无关节囊折叠的关节囊移位均能够恢复旋转,与完整关节囊相比无显著差异(P >.05)。在修复结构中,端端修复与关节囊移位联合折叠之间的活动范围存在显著差异(P <.05)。
在所有位置,关节囊切开后旋转运动均显著增加。关节囊闭合能够恢复与完整关节囊相似的旋转。关节囊移位与折叠联合应用可能为髋关节微不稳定情况提供更受限的旋转,但可能会对无松弛的髋关节造成过度限制。
对于髋关节松弛和微不稳定的患者,可能需要更先进的闭合技术或技术组合。同时,对于没有这些情况的患者,简单修复可能就足够了。