Chaney Amanda
Department of Transplant, College of Medicine, Mayo Clinic, Jacksonville, FL, USA.
Clin Exp Gastroenterol. 2021 Oct 5;14:385-396. doi: 10.2147/CEG.S323778. eCollection 2021.
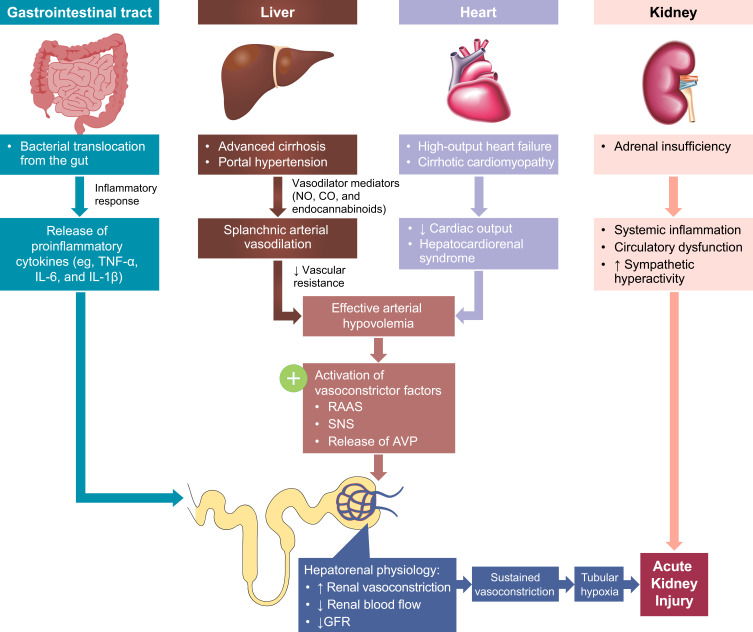
The hepatorenal syndrome type of acute kidney injury (HRS-AKI), formerly known as type 1 hepatorenal syndrome, is a rapidly progressing renal failure that occurs in many patients with advanced cirrhosis and ascites. Accumulating evidence has led to a recent evolution of diagnostic criteria for this serious complication of end-stage liver disease. The aim of this review is to provide an overview of disease-related characteristics and therapeutic management of patients with HRS-AKI. Relevant literature was compiled to support discussion of the pathophysiology, diagnosis, prognosis, associated conditions, prevention, treatment, and management of HRS-AKI. Onset of HRS-AKI is characterized by sudden severe renal vasoconstriction, leading to an acute reduction in glomerular filtration rate and rapid, potentially life-threatening, renal deterioration. Although our understanding of disease pathophysiology continues to evolve, etiology of HRS-AKI likely involves systemic hemodynamic changes caused by liver disease, inflammation, and damage to renal parenchyma. There is currently no gold standard for diagnosis, which typically involves a clinical workup, abdominal imaging, and laboratory assessments. The current consensus definition of HRS-AKI includes proposed diagnostic criteria based on changes in serum creatinine levels tailored for high sensitivity, and rapid detection to accelerate diagnosis and treatment initiation. The only potential cure for HRS-AKI is liver transplantation; however, vasoconstrictive agents and other supportive measures are used as needed to help maintain survival for patients who are awaiting or are ineligible for transplantation. The severity of HRS-AKI, complex pathology, limited treatment options, and range of associated conditions pose significant challenges for both patients and care providers.
肝肾综合征型急性肾损伤(HRS-AKI),以前称为1型肝肾综合征,是一种快速进展的肾衰竭,发生在许多晚期肝硬化和腹水患者中。越来越多的证据导致了这种终末期肝病严重并发症诊断标准的最新演变。本综述的目的是概述HRS-AKI患者的疾病相关特征和治疗管理。收集了相关文献,以支持对HRS-AKI的病理生理学、诊断、预后、相关病症、预防、治疗和管理的讨论。HRS-AKI的发作以突然严重的肾血管收缩为特征,导致肾小球滤过率急性降低,并迅速出现可能危及生命的肾功能恶化。尽管我们对疾病病理生理学的理解不断发展,但HRS-AKI的病因可能涉及由肝病、炎症和肾实质损伤引起的全身血流动力学变化。目前尚无诊断的金标准,通常包括临床检查、腹部影像学检查和实验室评估。HRS-AKI的当前共识定义包括基于血清肌酐水平变化提出的诊断标准,以实现高敏感性和快速检测,从而加速诊断和开始治疗。HRS-AKI的唯一潜在治愈方法是肝移植;然而,血管收缩剂和其他支持措施根据需要使用,以帮助等待移植或不符合移植条件的患者维持生命。HRS-AKI的严重性、复杂的病理、有限的治疗选择以及一系列相关病症给患者和护理人员都带来了重大挑战。