Tacelli Matteo, Petrone Maria Chiara, Capurso Gabriele, Muffatti Francesca, Andreasi Valentina, Partelli Stefano, Doglioni Claudio, Falconi Massimo, Arcidiacono Paolo Giorgio
Division of Pancreato-Biliary Endoscopy and EUS, Pancreas Translational and Clinical Research Center, San Raffaele Scientific Institute IRCCS, Milano, Italy.
Division of Pancreatic Surgery, Pancreas Translational and Clinical Research Center, San Raffaele Scientific Institute IRCCS, Milano, Italy.
Endosc Ultrasound. 2021 Sep-Oct;10(5):372-380. doi: 10.4103/EUS-D-20-00261.
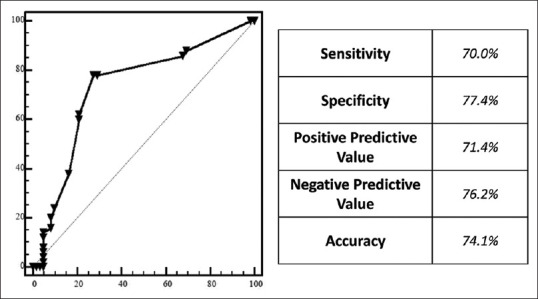
Prognosis of pancreatic neuroendocrine neoplasms (PanNENs) mostly depend on tumor stage and grade, determined by Ki-67 labeling index. EUS-FNA is considered the gold-standard technique to obtain it. The aims of our study were to establish diagnostic accuracy of preoperative EUS-FNA Ki-67 evaluation considering final pathological assessment on surgical specimen as gold standard and to investigate the possible impact on prognosis of misclassification.
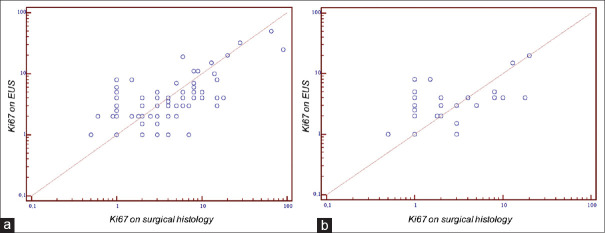
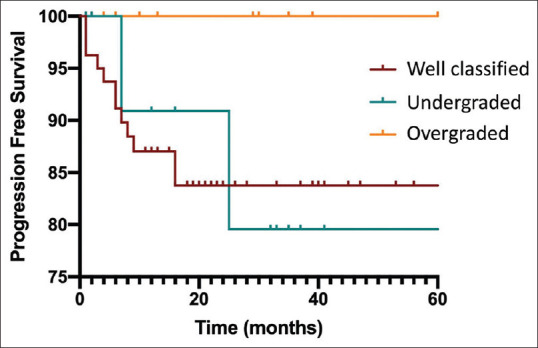
This is a retrospective study from a prospectively collected database. EUS-FNA grading (eG) and surgical one (sG) measured according to Ki-67 proliferative index values, according to 2017 WHO classification, were compared. eG-sG correlation was evaluated by Spearman index. Logistic regression investigated factors associated with misclassification. Prognostic difference in terms of progression-free survival was evaluated by Kaplan Meier method.
One hundred and twelve PanNENs patients enrolled. In 13.4% of patients (15/112) EUS-FNA "undergraded" patients (eG1 vs. sG2), while in 12.5% (n = 14) it "overgraded" PanNENs (eG2 to sG1). No misclassifications in G3 patients. In patients with tumors <20 mm (n = 44), 2 (4.5%) eG1 and 10 (22.7%) eG2 were finally classified respectively as G2 and G1 at surgical histology. No factors, as i.e. the lesions' size or their morphological aspect, were associated with misclassification. In overgraded PanNENs, no progression occurred, while in patients correctly classified/undergraded the progression rate was 14.3%.
This is the largest cohort of surgical PanNENs with preoperative EUS-FNA grading evaluation. Despite an acceptable eG-sG correlation, about 25% of patients are misclassified. Clinical impact of misclassification should be carefully considered especially in small tumors undergoing observation.
胰腺神经内分泌肿瘤(PanNENs)的预后主要取决于肿瘤分期和分级,这由Ki-67标记指数决定。超声内镜引导下细针穿刺抽吸活检(EUS-FNA)被认为是获取该指标的金标准技术。我们研究的目的是以手术标本的最终病理评估为金标准,确定术前EUS-FNA对Ki-67评估的诊断准确性,并调查分类错误对预后的可能影响。
这是一项基于前瞻性收集数据库的回顾性研究。根据2017年世界卫生组织分类,比较了根据Ki-67增殖指数值测量的EUS-FNA分级(eG)和手术分级(sG)。通过Spearman指数评估eG与sG的相关性。逻辑回归分析与分类错误相关的因素。采用Kaplan-Meier法评估无进展生存期方面的预后差异。
纳入112例PanNENs患者。13.4%的患者(15/112)EUS-FNA对患者“分级过低”(eG1对sG2),而12.5%(n = 14)的患者EUS-FNA对PanNENs“分级过高”(eG2至sG1)。G3患者无分类错误。在肿瘤<20 mm的患者(n = 44)中,2例(4.5%)eG1和10例(22.7%)eG2最终在手术组织学上分别被分类为G2和G1。没有因素,如病变大小或形态,与分类错误相关。在分级过高的PanNENs中,未发生进展,而在正确分类/分级过低的患者中,进展率为14.3%。
这是最大的一组接受术前EUS-FNA分级评估的手术切除PanNENs队列。尽管eG与sG有可接受的相关性,但约25%的患者被错误分类。分类错误的临床影响应仔细考虑,尤其是在接受观察的小肿瘤患者中。