Division of Surgical Oncology, Department of Surgery, University of Colorado School of Medicine, Aurora.
Department of Hepatobiliary and Pancreatic Surgery, Graduate School of Medicine, Tokyo Medical and Dental University, Tokyo, Japan.
JAMA Netw Open. 2023 Mar 1;6(3):e234096. doi: 10.1001/jamanetworkopen.2023.4096.
The number of patients with small nonfunctional pancreatic neuroendocrine tumors (NF-PanNETs) is increasing. However, the role of surgery for small NF-PanNETs remains unclear.
To evaluate the association between surgical resection for NF-PanNETs measuring 2 cm or smaller and survival.
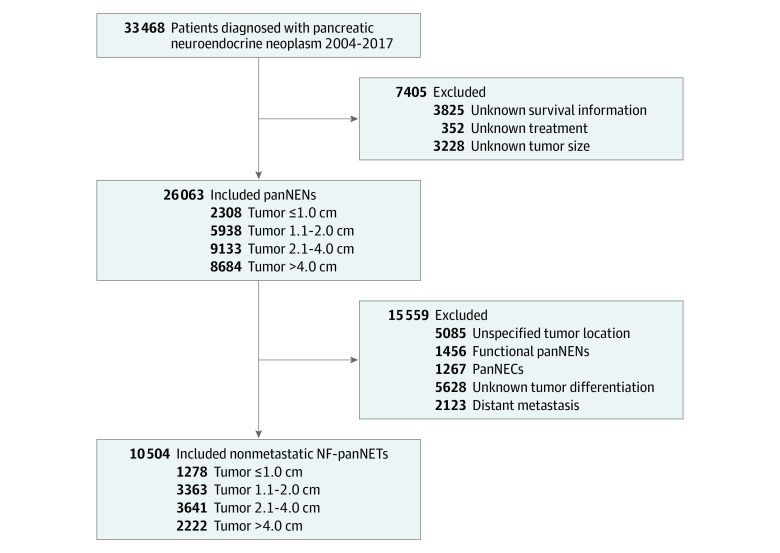
DESIGN, SETTING, AND PARTICIPANTS: This cohort study used data from the National Cancer Database and included patients with NF-pancreatic neuroendocrine neoplasms who were diagnosed between January 1, 2004, and December 31, 2017. Patients with small NF-PanNETs were divided into 2 groups: group 1a (tumor size, ≤1 cm) and group 1b (tumor size, 1.1-2.0 cm). Patients without information on tumor size, overall survival, and surgical resection were excluded. Data analysis was performed in June 2022.
Patients with vs without surgical resection.
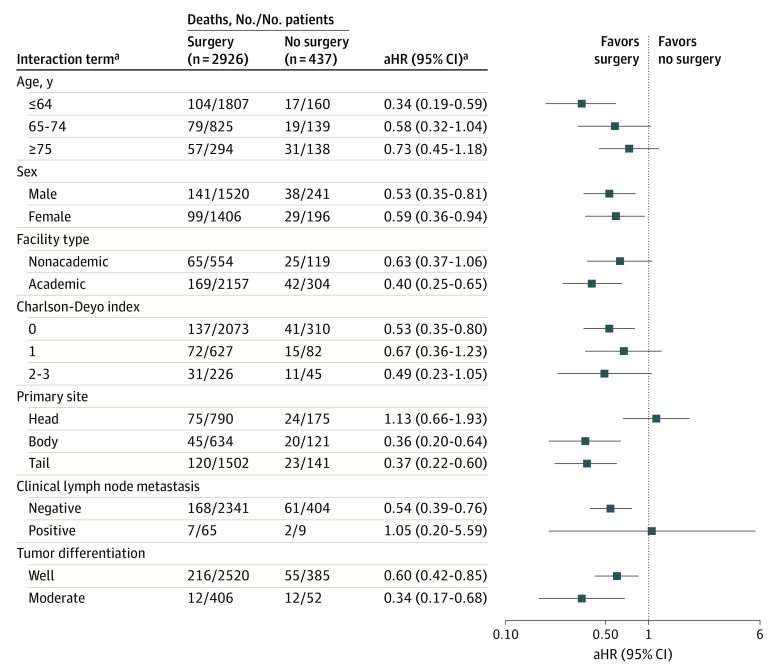
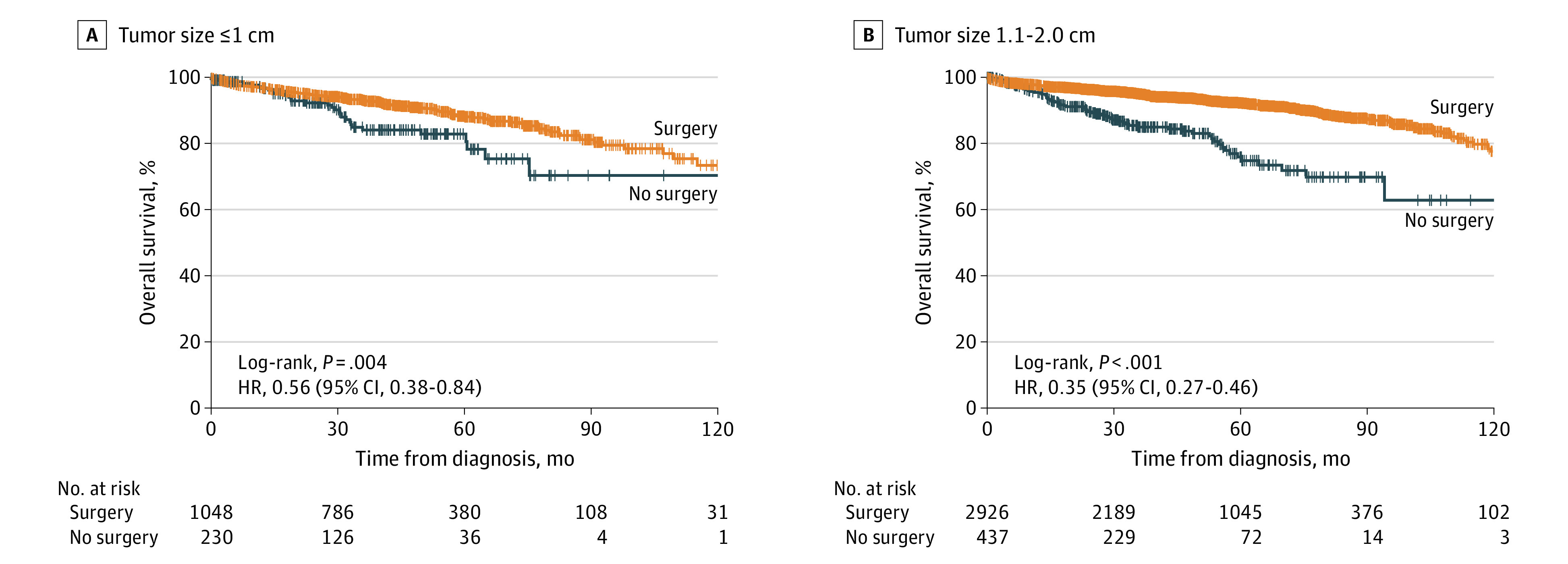
The primary outcome was overall survival of patients in group 1a or group 1b who underwent surgical resection compared with those who did not, which was evaluated using Kaplan-Meier estimates and multivariable Cox proportional hazards regression models. Interactions between preoperative factors and surgical resection were analyzed with a multivariable Cox proportional hazards regression model.
Of the 10 504 patients with localized NF-PanNETs identified, 4641 were analyzed. These patients had a mean (SD) age of 60.5 (12.7) years and included 2338 males (50.4%). The median (IQR) follow-up time was 47.1 (28.2-71.6) months. In total, 1278 patients were in group 1a and 3363 patients were in group 1b. The surgical resection rates were 82.0% in group 1a and 87.0% in group 1b. After adjustment for preoperative factors, surgical resection was associated with longer survival for patients in group 1b (hazard ratio [HR], 0.58; 95% CI, 0.42-0.80; P < .001) but not for patients in group 1a (HR, 0.68; 95% CI, 0.41-1.11; P = .12). In group 1b, interaction analysis found that age of 64 years or younger, absence of comorbidities, treatment at academic institutions, and distal pancreatic tumors were factors associated with increased survival after surgical resection.
Findings of this study support an association between surgical resection and increased survival in select patients with NF-PanNETs measuring 1.1 to 2.0 cm who were younger than 65 years, had no comorbidities, received treatment at academic institutions, and had tumors of the distal pancreas. Future investigations of surgical resection for small NF-PanNETs that include the Ki-67 index are warranted to validate these findings.
患有小的无功能性胰腺神经内分泌肿瘤(NF-PanNETs)的患者数量正在增加。然而,对于小 NF-PanNETs 的手术治疗作用仍不清楚。
评估 NF-PanNETs 直径为 2cm 或更小的手术切除与生存之间的关系。
设计、设置和参与者:本队列研究使用了国家癌症数据库的数据,纳入了 2004 年 1 月 1 日至 2017 年 12 月 31 日期间诊断为 NF-胰腺神经内分泌肿瘤的患者。将小 NF-PanNETs 患者分为 2 组:组 1a(肿瘤大小,≤1cm)和组 1b(肿瘤大小,1.1-2.0cm)。排除了肿瘤大小、总生存期和手术切除信息缺失的患者。数据分析于 2022 年 6 月进行。
有手术切除和无手术切除的患者。
主要结局是接受手术切除的组 1a 或组 1b 患者与未接受手术切除的患者的总生存期,使用 Kaplan-Meier 估计和多变量 Cox 比例风险回归模型进行评估。使用多变量 Cox 比例风险回归模型分析术前因素与手术切除之间的相互作用。
在确定的 10504 例局限性 NF-PanNETs 患者中,对 4641 例患者进行了分析。这些患者的平均(SD)年龄为 60.5(12.7)岁,包括 2338 名男性(50.4%)。中位(IQR)随访时间为 47.1(28.2-71.6)个月。共有 1278 例患者在组 1a,3363 例患者在组 1b。手术切除率在组 1a 为 82.0%,在组 1b 为 87.0%。在调整了术前因素后,手术切除与组 1b 患者的生存延长相关(HR,0.58;95%CI,0.42-0.80;P<0.001),但与组 1a 患者无关(HR,0.68;95%CI,0.41-1.11;P=0.12)。在组 1b 中,交互分析发现,年龄在 64 岁以下、无合并症、在学术机构接受治疗和胰腺远端肿瘤是手术切除后生存延长的相关因素。
本研究的结果支持在年龄在 65 岁以下、无合并症、在学术机构接受治疗和胰腺远端肿瘤的选择患者中,手术切除与 NF-PanNETs 直径为 1.1-2.0cm 的患者的生存增加之间存在关联。需要进一步研究包括 Ki-67 指数在内的小 NF-PanNETs 的手术切除,以验证这些发现。