Department of Pharmacy Practice, School of Pharmacy and Pharmaceutical Sciences, University at Buffalo, Buffalo, NY, USA.
BMC Public Health. 2021 Oct 23;21(1):1922. doi: 10.1186/s12889-021-11987-z.
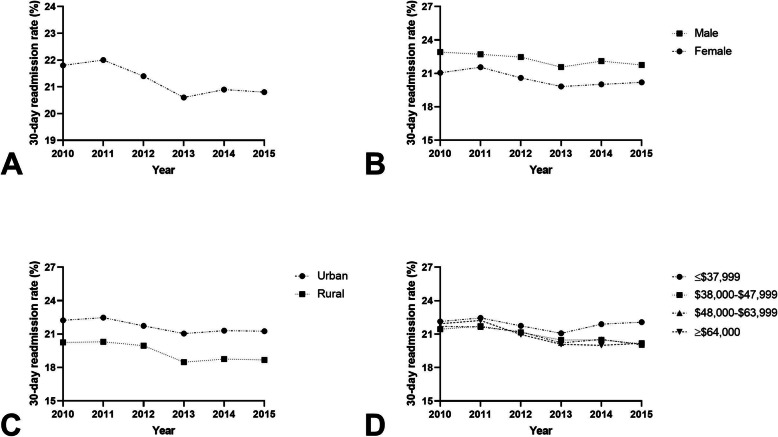
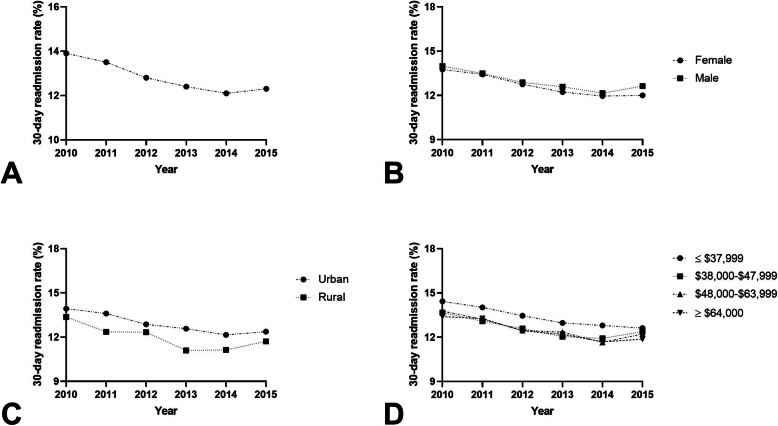
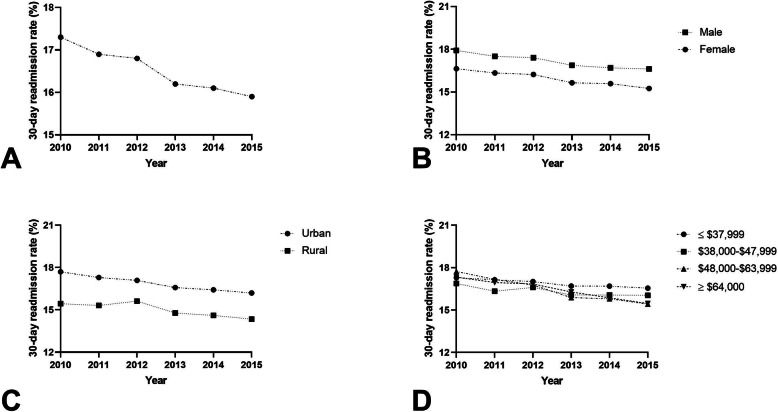
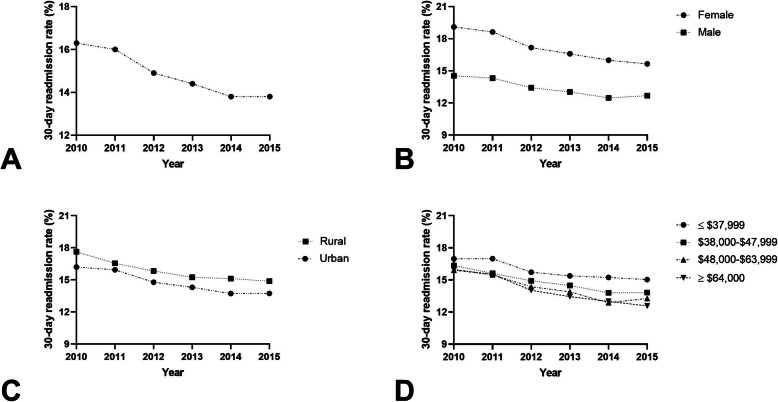
Early hospital readmissions remain common in patients with conditions targeted by the CMS Hospital Readmission Reduction Program (HRRP). There is still no consensus on whether readmission measures should be adjusted based on social factors, and there are few population studies within the U.S. examining how social characteristics influence readmissions for HRRP-targeted conditions. The objective of this study was to determine if specific socio-demographic and -economic factors are associated with 30-day readmissions in HRRP-targeted conditions: acute exacerbation of chronic obstructive pulmonary disease, pneumonia, acute myocardial infarction, and heart failure.
The Nationwide Readmissions Database was used to identify patients admitted with HRRP-targeted conditions between January 1, 2010 and September 30, 2015. Stroke was included as a control condition because it is not included in the HRRP. Multivariate models were used to assess the relationship between three social and economic characteristics (gender, urban/rural hospital designation, and estimated median household income within the patient's zip code) and 30-day readmission rates using a hierarchical two-level logistic model. Age-adjusted models were used to assess relationship differences between Medicare vs. non-Medicare populations.
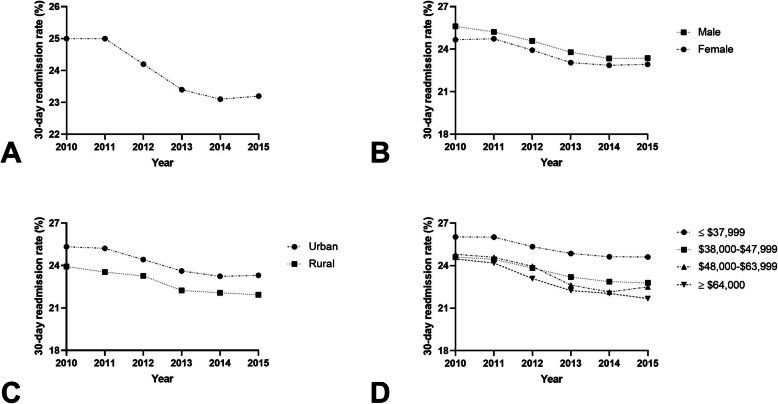
There were 19,253,997 weighted index hospital admissions for all diagnoses and 3,613,488 30-day readmissions between 2010 and 2015. Patients in the lowest income quartile (≤$37,999) had an increased odds of 30-day readmission across all conditions (P < 0.0001). Female gender and rural hospital designation were associated with a decreased odds of 30-day readmission for most targeted conditions (P < 0.05). Similar findings were also seen in patients ≥65 years old.
Socio-demographic and -economic factors are associated with 30-day readmission rates and should be incorporated into tools or interventions to improve discharge planning and mitigate against readmission.
在美国,针对 CMS 医院再入院减少计划(HRRP)目标的疾病,患者早期再次住院仍然很常见。目前仍然没有共识认为是否应根据社会因素调整再入院措施,而且很少有针对 HRRP 目标疾病的人群研究来检查社会特征如何影响再入院率。本研究的目的是确定特定的社会人口统计学和社会经济学因素是否与 HRRP 目标疾病的 30 天再入院率相关:慢性阻塞性肺疾病急性加重、肺炎、急性心肌梗死和心力衰竭。
使用全国再入院数据库,确定 2010 年 1 月 1 日至 2015 年 9 月 30 日期间因 HRRP 目标疾病入院的患者。将中风纳入对照疾病,因为它不包括在 HRRP 中。使用多变量模型,通过分层两水平逻辑模型,使用三个社会经济特征(性别、城乡医院分类和患者邮政编码内的估计中位数家庭收入)评估 30 天再入院率与 30 天再入院率之间的关系。使用年龄调整模型评估医疗保险与非医疗保险人群之间的关系差异。
在 2010 年至 2015 年期间,所有诊断的加权指数医院入院人数为 19253997 人,30 天再入院人数为 3613488 人。在所有条件下,收入最低四分位数(≤37999 美元)的患者 30 天再入院的可能性增加(P <0.0001)。女性性别和农村医院分类与大多数目标疾病的 30 天再入院率降低相关(P <0.05)。在年龄≥65 岁的患者中也观察到类似的发现。
社会人口统计学和社会经济学因素与 30 天再入院率相关,应将其纳入工具或干预措施中,以改善出院计划并减轻再入院率。