Henson Sian M, Aksentijevic Dunja
Centre for Translational Medicine and Therapeutics, London, United Kingdom.
Centre for Biochemical Pharmacology, London, United Kingdom.
Front Pharmacol. 2021 Oct 7;12:716517. doi: 10.3389/fphar.2021.716517. eCollection 2021.
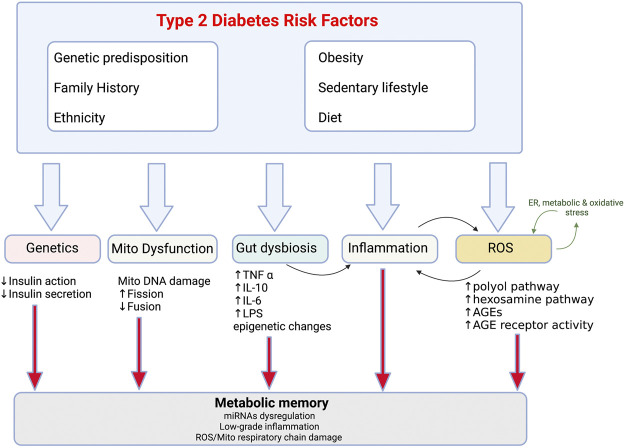
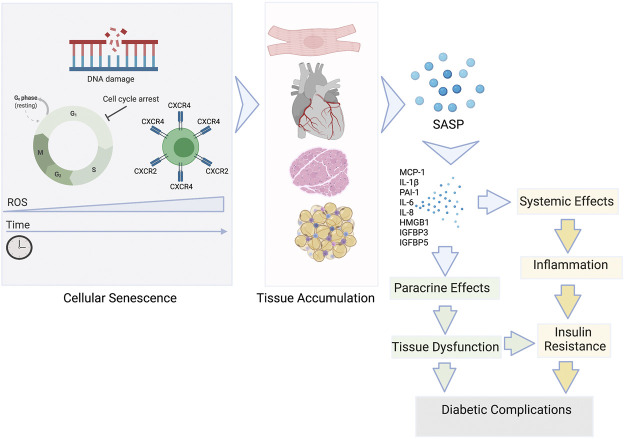
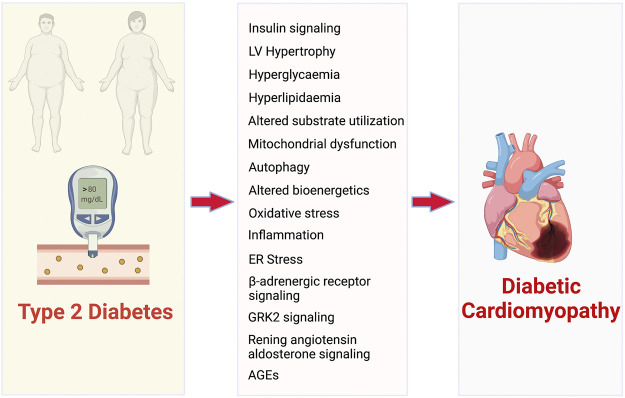
Inflammation is well understood to be a physiological process of ageing however it also underlies many chronic diseases, including conditions without an obvious pathogenic inflammatory element. Recent findings have unequivocally identified type 2 diabetes (T2D) as a chronic inflammatory disease characterized by inflammation and immune senescence. Immunosenescence is a hallmark of the prolonged low-grade systemic inflammation, in particular associated with metabolic syndrome and can be a cause as well as a consequence of T2D. Diabetes is a risk factor for cardiovascular mortality and remodelling and with particular changes to myocardial structure, function, metabolism and energetics collectively resulting in diabetic cardiomyopathy. Both cardiomyocytes and immune cells undergo metabolic remodelling in T2D and as a result become trapped in a vicious cycle of lost metabolic flexibility, thus losing their key adaptive mechanisms to dynamic changes in O and nutrient availability. Immunosenescence driven by metabolic stress may be both the cause and key contributing factor to cardiac dysfunction in diabetic cardiomyopathy by inducing metabolic perturbations that can lead to impaired energetics, a strong predictor of cardiac mortality. Here we review our current understanding of the cross-talk between inflammaging and cardiomyocytes in T2D cardiomyopathy. We discuss potential mechanisms of metabolic convergence between cell types which, we hypothesize, might tip the balance between resolution of the inflammation versus adverse cardiac metabolic remodelling in T2D cardiomyopathy. A better understanding of the multiple biological paradigms leading to T2D cardiomyopathy including the immunosenescence associated with inflammaging will provide a powerful target for successful therapeutic interventions.
炎症被公认为是衰老的一种生理过程,但它也是许多慢性疾病的基础,包括一些没有明显致病性炎症因素的病症。最近的研究结果明确地将2型糖尿病(T2D)确定为一种以炎症和免疫衰老为特征的慢性炎症性疾病。免疫衰老是长期低度全身性炎症的一个标志,尤其与代谢综合征相关,并且可能是T2D的一个原因及后果。糖尿病是心血管疾病死亡率和重塑的一个风险因素,特别是会导致心肌结构、功能、代谢和能量学的特定变化,这些共同导致糖尿病心肌病。在T2D中,心肌细胞和免疫细胞都会经历代谢重塑,结果陷入代谢灵活性丧失的恶性循环,从而失去它们应对氧气和营养物质供应动态变化的关键适应机制。由代谢应激驱动的免疫衰老可能通过引发代谢紊乱导致能量学受损(这是心脏死亡率的一个重要预测指标),从而成为糖尿病性心肌病心脏功能障碍的原因和关键促成因素。在此,我们回顾对T2D心肌病中炎症衰老与心肌细胞之间相互作用的当前理解。我们讨论细胞类型之间代谢趋同的潜在机制,我们推测这些机制可能会打破T2D心肌病中炎症消退与不良心脏代谢重塑之间的平衡。更好地理解导致T2D心肌病的多种生物学模式,包括与炎症衰老相关的免疫衰老,将为成功的治疗干预提供一个有力靶点。