Fransson Marcus, Helldén Anders, Östholm Balkhed Åse, Nezirević Dernroth Dženeta, Ha Maria, Haglund Mats, Milos Peter, Hanberger Håkan, Kågedal Bertil
Department of Neurosurgery and Department of Biomedical and Clinical Sciences, Linköping University, Linköping, Sweden.
Department of Clinical Chemistry and Clinical Pharmacology and Department of Biomedical and Clinical Sciences, Linköping University, Linköping, Sweden.
Front Pharmacol. 2021 Oct 6;12:728075. doi: 10.3389/fphar.2021.728075. eCollection 2021.
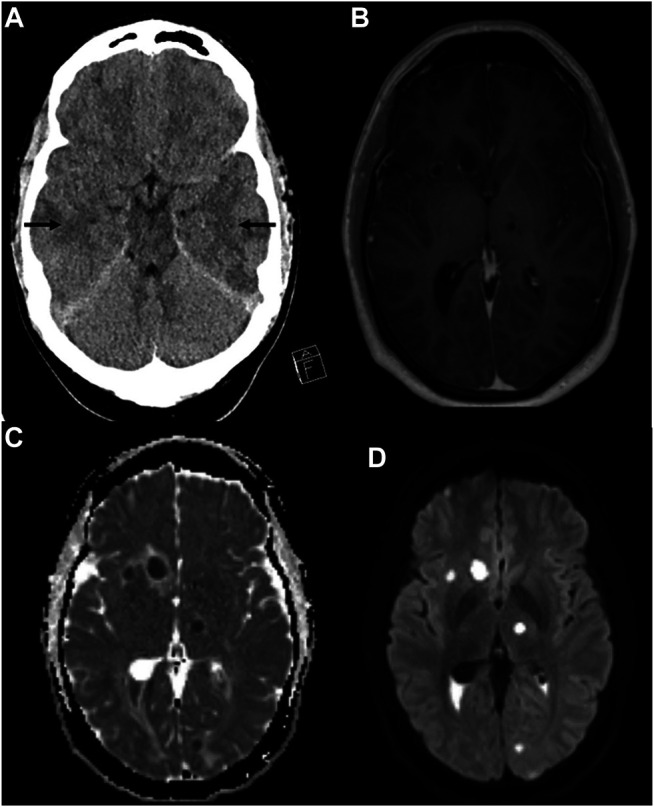
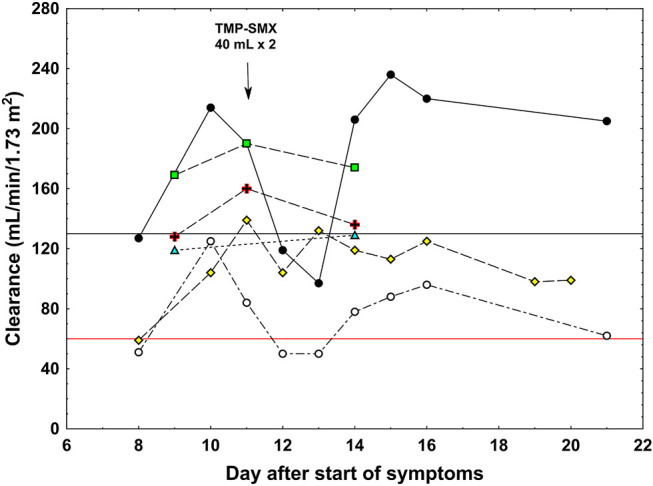
occasionally causes brain abscesses that can be life-threatening, requiring prompt antibiotic and neurosurgical treatment. The source is often dental, and it may spread to the eye or the brain parenchyma. We report the case of a 34-year-old man with signs of apical periodontitis, endophthalmitis, and multiple brain abscesses caused by . Initial treatment with meropenem and vancomycin was unsuccessful due to subtherapeutic concentrations, despite recommended dosages. Adequate concentrations could be reached only after increasing the dose of meropenem to 16 g/day and vancomycin to 1.5 g × 4. The patient exhibited high creatinine clearance consistent with augmented renal clearance, although iohexol and cystatin C clearances were normal. Plasma free vancomycin clearance followed that of creatinine. A one-day dose of trimethoprim-sulfamethoxazole led to an increase in serum creatinine and a decrease in both creatinine and urea clearances. These results indicate that increased tubular secretion of the drugs was the cause of suboptimal antibiotic treatment. The patient eventually recovered, but his left eye needed enucleation. Our case illustrates that augmented renal clearance can jeopardize the treatment of serious bacterial infections and that high doses of antibiotics are needed to achieve therapeutic concentrations in such cases. The mechanisms for regulation of kidney tubular transporters of creatinine, urea, vancomycin, and meropenem in critically ill patients are discussed.
偶尔会引发可危及生命的脑脓肿,这需要及时进行抗生素及神经外科治疗。其感染源通常来自牙科,且可能扩散至眼部或脑实质。我们报告了一例34岁男性病例,其患有根尖周炎、眼内炎及由……引起的多发性脑脓肿。尽管给予了推荐剂量,但最初使用美罗培南和万古霉素治疗因药物浓度未达治疗水平而失败。仅在将美罗培南剂量增至16g/天且万古霉素增至1.5g×4后才达到足够浓度。尽管碘海醇和胱抑素C清除率正常,但患者肌酐清除率较高,提示存在肾脏清除率增加。血浆游离万古霉素清除率与肌酐清除率一致。单剂量的甲氧苄啶 - 磺胺甲恶唑导致血清肌酐升高,肌酐和尿素清除率均下降。这些结果表明药物肾小管分泌增加是抗生素治疗效果欠佳的原因。患者最终康复,但左眼需要摘除。我们的病例表明肾脏清除率增加可能危及严重细菌感染的治疗,在此类情况下需要高剂量抗生素才能达到治疗浓度。文中还讨论了重症患者中肌酐、尿素、万古霉素及美罗培南肾小管转运体的调节机制。