From the Department of Neurology (M.D., M.S., J.D., H.T., J.L.), Ulm University; Department of Neurosurgery (M.D.), University Hospital Tübingen; Neuroimmunology (G.N., K.-P.W., F.L.), Institute of Clinical Chemistry, University Hospital Schleswig-Holstein Kiel/Lübeck; Department of Neurology (K.-W.S., P.S.), Hannover Medical School; Department of Neurology (C.G.), University Hospital Jena; Department of Neurology (M.R., H.-P.H., N.M.), Medical Faculty, Heinrich Heine University Düsseldorf; Department of Neurology (M.R.), Center for Neurology and Neuropsychiatry, LVR-Klinikum Düsseldorf, Düsseldorf; Institute of Neuroimmunology and Multiple Sclerosis (M.A.F., M.K.), University Medical Center Hamburg-Eppendorf; Department of Neurology (M.P.M., M.M.), University of Cologne, Faculty of Medicine and University Hospital; Institute of Clinical Neuroimmunology (F.S.T., T.K.), University Hospital and Biomedical Center, Ludwig-Maximilians University Munich; Department of Pediatrics (M.G.H.), University Hospital RWTH Aachen; Technische Universität Dresden (H.S.), and Department of Neurology, University Hospital Augsburg; Department of Neurology (F.T.B.), University Hospital Leipzig; Department of Neurology (C.K.), Klinikum Osnabrück; Department of Neurology (U.K.Z.), Section for Neuroimmunology, University Hospital Rostock; Department of Neurology with Institute of Translational Neurology (N.M., C.C.G.), University Hospital Münster; Department of Neurology (P.L.), University Hospital Göttingen; Institute of Epidemiology and Medical Biometry, Ulm University; and Department of Neurology (F.L.), University Hospital Schleswig-Holstein and Kiel University, Germany.
Neurol Neuroimmunol Neuroinflamm. 2021 Oct 25;8(6). doi: 10.1212/NXI.0000000000001086. Print 2021 Nov.
CSF in antibody-defined autoimmune encephalitis (AE) subtypes shows subtype-dependent degrees of inflammation ranging from rare and often mild to frequent and often robust. AEs with NMDA receptor antibodies (NMDAR-E) and leucine-rich glioma-inactivated protein 1 antibodies (LGI1-E) represent opposite ends of this spectrum: NMDAR-E with typically frequent/robust and LGI1-E with rare/mild CSF inflammation. For a more in-depth analysis, we characterized CSF findings in acute, therapy-naive NMDAR-E and LGI1-E in a multicentric, retrospective, cross-sectional setting.
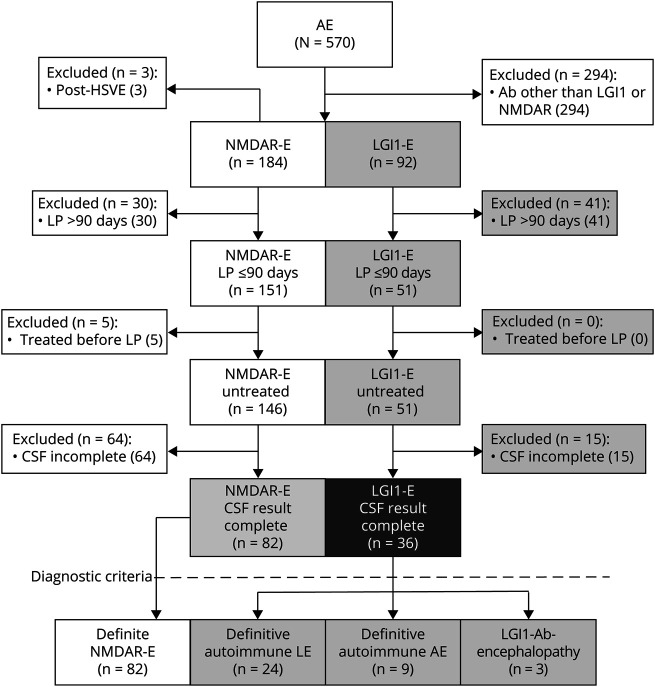
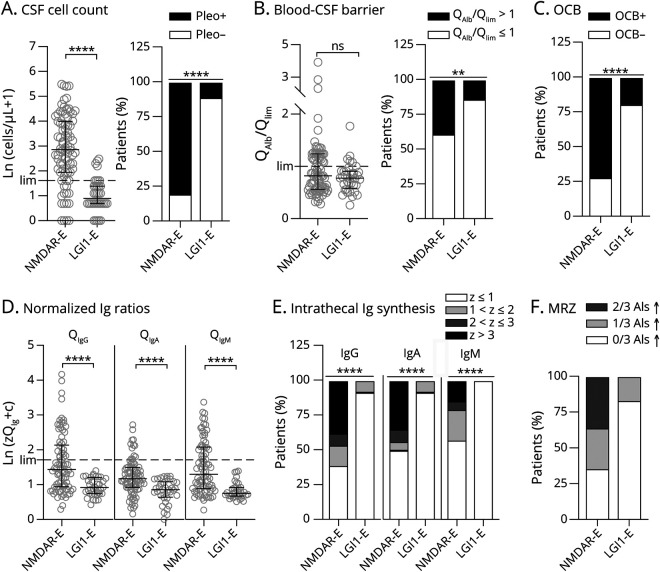
Eighty-two patients with NMDAR-E and 36 patients with LGI1-E from the GErman NEtwork for Research of AuToimmune Encephalitis (GENERATE) with lumbar puncture within 90 days of onset and before immunotherapy were included. CSF parameters comprised leukocytes, oligoclonal bands (OCBs), and CSF/serum ratios for albumin, immunoglobulin G (IgG), A (IgA), and M (IgM), the latter 3 converted to Z scores according to Reiber formulas. The MRZ reaction was tested in 14 patients with NMDAR-E and 6 patients with LGI1-E, respectively.
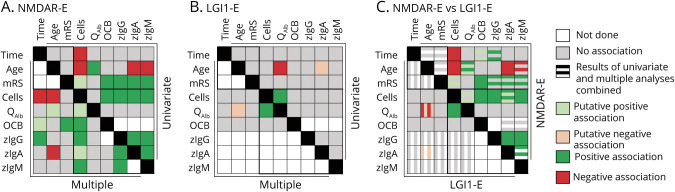
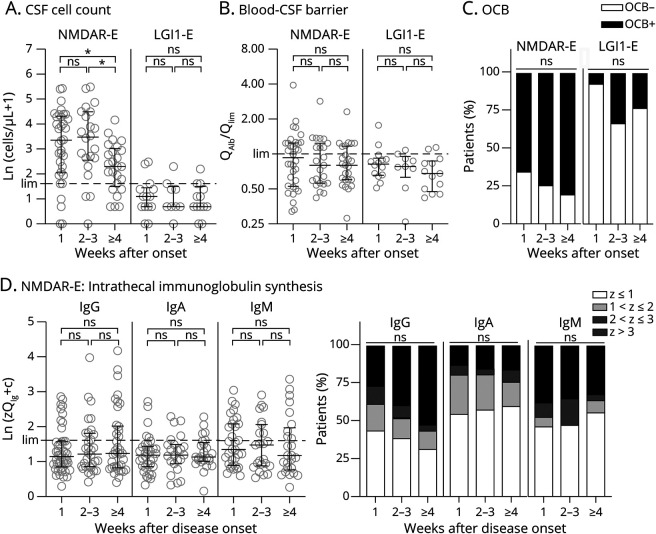
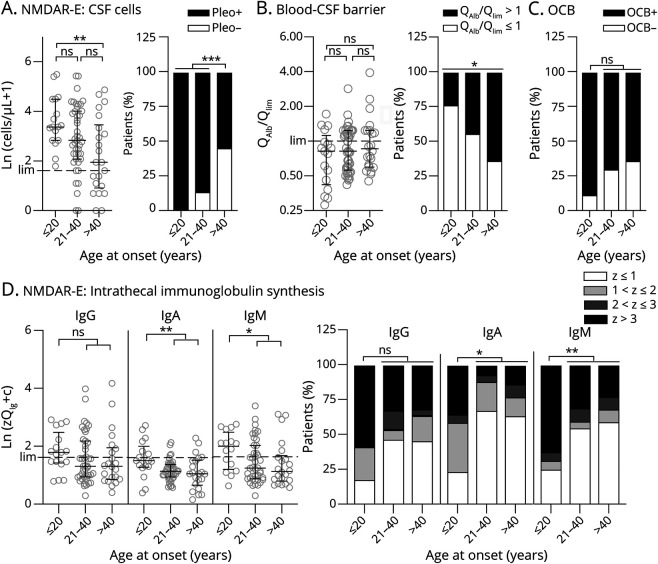
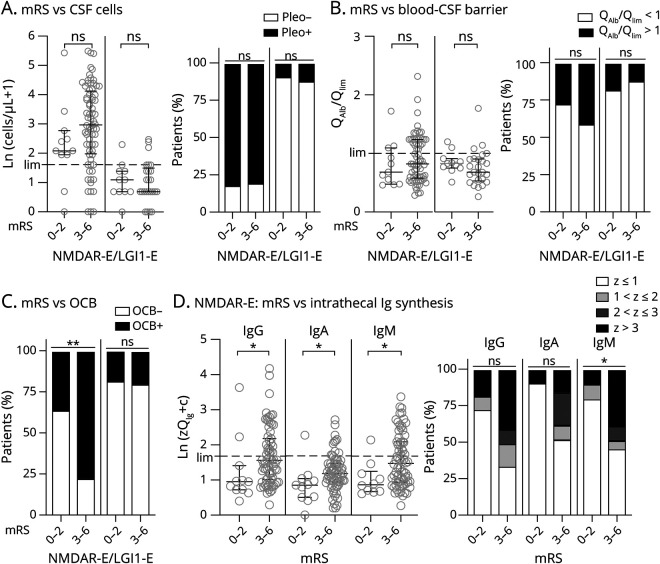
CSF was abnormal in 94% of NMDAR-E but only in 36% of LGI1-E patients. Robust quantitative intrathecal immunoglobulin synthesis (IIS, IgG > IgM >> IgA) was characteristic for NMDAR-E, but absent in LGI-E. In NMDAR-E, CSF leukocytes were higher when IIS was present or more pronounced. In addition, in NMDAR-E, CSF leukocytes were lower and IIS occurred less often and if so to a lesser degree at older age. Patients with NMDAR-E with severe functional impairment more often had positive OCBs. In CSF obtained later than 3 weeks of onset, leukocytes were lower. In parallel, the correlation of leukocytes with IIS disappeared as IIS was partially independent of disease duration. The MRZ reaction was positive in 5 (36%) patients with NMDAR-E. All these associations were completely absent in LGI1-E. Here, younger patients showed more blood-CSF barrier dysfunction. In LGI1-E, but not in NMDAR-E, the blood-CSF barrier was more dysfunctional when CSF leukocytes were higher.
NMDAR-E and LGI-E differ in their typical extent of CSF inflammation. In addition, the patterns formed by the different inflammatory CSF parameters and their relationship with disease severity, age, and disease duration are subtype-characteristic. Moreover, signs for multiple sclerosis-like chronic inflammation are present in a subgroup of patients with NMDAR-E. These CSF patterns might be markers for the different immunopathogeneses of LGI1-E and NMDAR-E.
在抗体定义的自身免疫性脑炎(AE)亚型的脑脊液中,炎症程度存在亚型依赖性,从罕见且常为轻度到常见且常为重度不等。具有 N-甲基-D-天冬氨酸受体抗体(NMDAR-E)和富含亮氨酸胶质瘤失活蛋白 1 抗体(LGI1-E)的 AE 代表了该谱的两个极端:NMDAR-E 通常表现为频繁/重度炎症,而 LGI1-E 则表现为罕见/轻度炎症。为了进行更深入的分析,我们在一项多中心、回顾性、横断面研究中,对急性、未经治疗的 NMDAR-E 和 LGI1-E 患者的脑脊液发现进行了特征描述。
纳入了来自 GErman NEtwork for Research of AuToimmune Encephalitis(GENERATE)的 82 例 NMDAR-E 患者和 36 例 LGI1-E 患者,他们在发病后 90 天内并在免疫治疗前接受了腰椎穿刺。脑脊液参数包括白细胞、寡克隆带(OCB)以及白蛋白、免疫球蛋白 G(IgG)、A(IgA)和 M(IgM)的脑脊液/血清比值,后三者根据 Reiber 公式转换为 Z 分数。在 14 例 NMDAR-E 患者和 6 例 LGI1-E 患者中分别检测了 MRZ 反应。
94%的 NMDAR-E 患者的脑脊液异常,而只有 36%的 LGI1-E 患者的脑脊液异常。NMDAR-E 的特征是强烈的定量鞘内免疫球蛋白合成(IIS,IgG>IgM>>IgA),而 LGI-E 则不存在。在 NMDAR-E 中,如果存在 IIS 或 IIS 更明显,脑脊液白细胞更高。此外,在 NMDAR-E 中,白细胞较低,IIS 发生的频率和程度较低,且随着年龄的增长而发生。具有严重功能损害的 NMDAR-E 患者更常出现阳性 OCB。在发病后 3 周以上获得的脑脊液中,白细胞更低。同时,白细胞与 IIS 的相关性消失,因为 IIS 部分独立于疾病持续时间。在 5(36%)例 NMDAR-E 患者中,MRZ 反应为阳性。所有这些关联在 LGI1-E 中完全不存在。在这里,年轻患者表现出更严重的血脑屏障功能障碍。在 LGI1-E 中,而不是在 NMDAR-E 中,当脑脊液白细胞更高时,血脑屏障的功能障碍更严重。
NMDAR-E 和 LGI-E 在脑脊液炎症的典型程度上存在差异。此外,不同炎症性脑脊液参数的模式及其与疾病严重程度、年龄和疾病持续时间的关系是亚型特征。此外,在 NMDAR-E 的一个亚组患者中存在类似于多发性硬化的慢性炎症迹象。这些脑脊液模式可能是 LGI1-E 和 NMDAR-E 不同免疫发病机制的标志物。