Department of Internal Medicine, Eastern Virginia Medical School, Norfolk, VA, USA.
Department of Medicine, Hospital of the University of Pennsylvania, Philadelphia, PA, USA.
Am J Case Rep. 2021 Oct 26;22:e933975. doi: 10.12659/AJCR.933975.
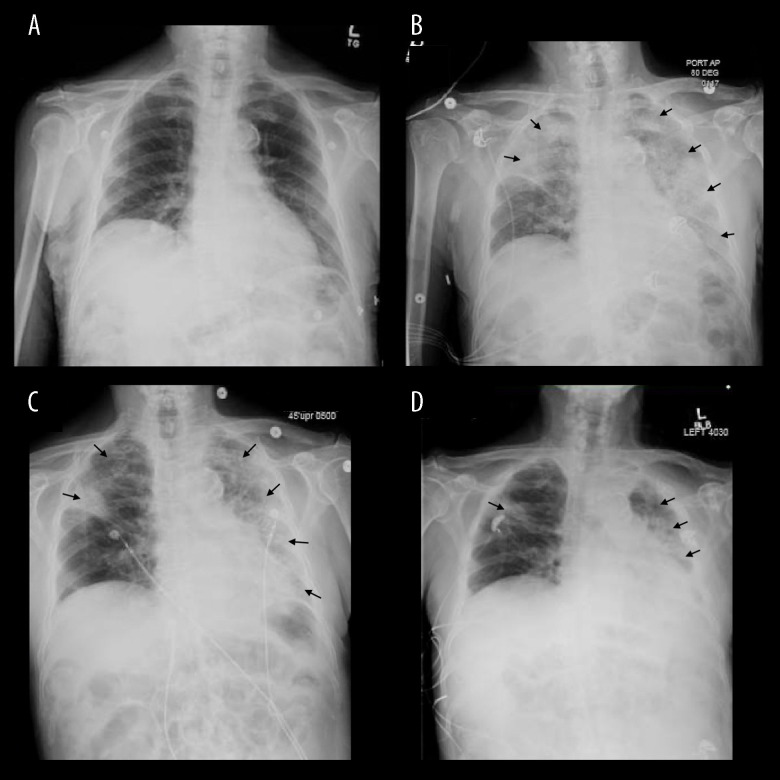
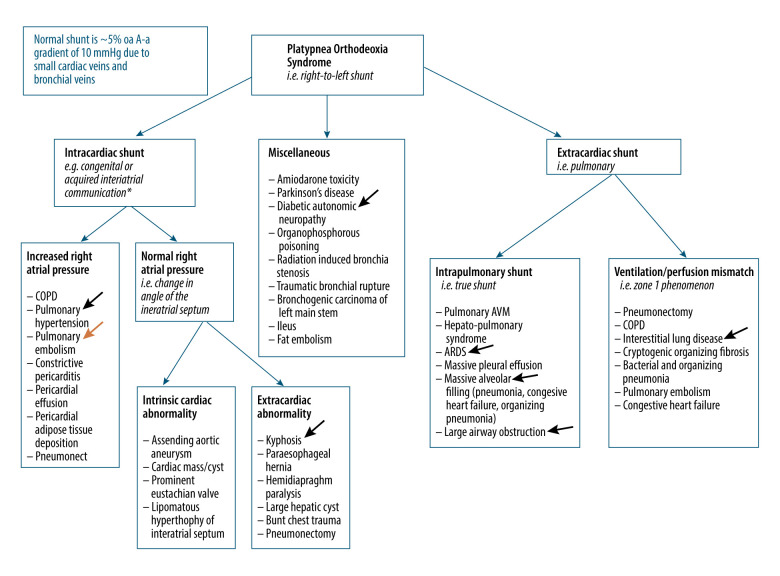
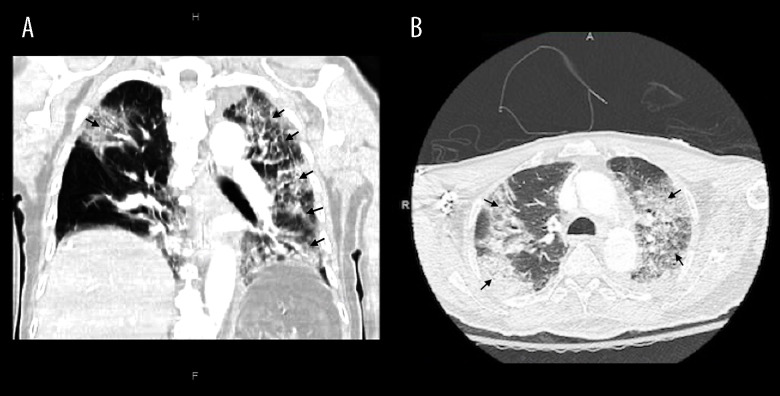
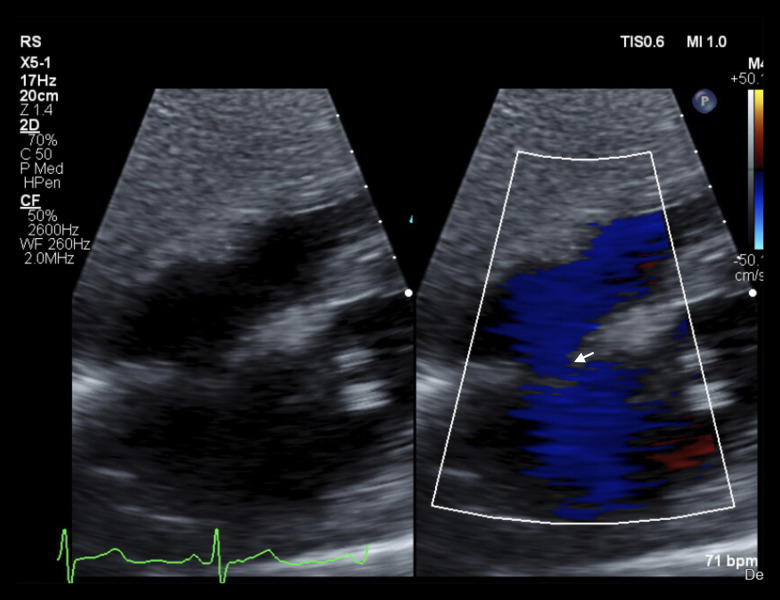
BACKGROUND Platypnea orthodeoxia syndrome (POS) presents with positional dyspnea and hypoxemia defined as arterial desaturation of at least 5% or a drop in PaO2 of at least 4 mmHg. Causes of POS include a variety of cardiopulmonary etiologies and has been reported in patients recovering from severe COVID-19 pneumonia. However, clinical presentation and outcomes in a patient with multiple interrelated mechanisms of shunting has not been documented. CASE REPORT An 85-year-old man hospitalized for hypertensive emergency and severe COVID-19 pneumonia was diagnosed with platypnea orthodeoxia on day 28 of illness. During his disease course, the patient required supplemental oxygen by high-flow nasal cannula but never required invasive mechanical ventilation. Chest imaging revealed evolving mixed consolidation and ground-glass opacities with a patchy and diffuse distribution, involving most of the left lung. Echocardiography was ordered to evaluate for intracardiac shunt, which revealed a patent foramen ovale. Closure of the patent foramen ovale was not pursued. Management included graded progression to standing and supplemental oxygen increases when upright. The patient was discharged to a skilled nursing facility and his positional oxygen requirement resolved on approximately day 78. CONCLUSIONS The present case highlights the multiple interrelated mechanisms of shunting in patients with COVID-related lung disease and a patent foramen ovale. Eight prior cases of POS after COVID-19 pneumonia have been reported to date but none with a known patent foramen ovale. In patients with persistent positional oxygen requirements at follow-up, quantifying shunt fraction over time through multiple modalities can guide treatment decisions.
体位性呼吸困难-低氧血症(POS)的特点是体位性呼吸困难和低氧血症,定义为动脉血氧饱和度至少下降 5%或 PaO2 至少下降 4mmHg。POS 的病因包括多种心肺病因,并已在从严重 COVID-19 肺炎中恢复的患者中报告。然而,具有多种相关分流机制的患者的临床表现和结局尚未记录。
一名 85 岁男性因高血压急症和严重 COVID-19 肺炎住院,在发病第 28 天被诊断为体位性呼吸困难-低氧血症。在他的病程中,患者需要高流量鼻导管吸氧,但从未需要有创机械通气。胸部影像学显示进展性混合性实变和磨玻璃影,呈斑片状和弥漫性分布,累及左肺大部分。为评估心内分流而行超声心动图检查,显示卵圆孔未闭。未行卵圆孔未闭封堵术。治疗包括逐渐过渡到站立位和直立时增加补充氧气。患者出院至康复护理机构,体位性氧需求约在第 78 天得到解决。
本病例突出了 COVID 相关肺部疾病和卵圆孔未闭患者的多种相关分流机制。迄今为止,已报告了 8 例 COVID-19 肺炎后 POS,但均无已知卵圆孔未闭。在随访中持续存在体位性氧需求的患者中,通过多种方式随时间量化分流量可指导治疗决策。