Jiang Linhan, Tan Xiaoxia, Li Jun, Li Yaling
Department of Pharmacy, The Affiliated Hospital of Southwest Medical University, Luzhou, China.
School of Pharmacy, Southwest Medical University, Luzhou, China.
Front Oncol. 2021 Oct 12;11:726008. doi: 10.3389/fonc.2021.726008. eCollection 2021.
This study aims to inform previous clinical assessments to better understand the total risk of hypertension with atezolizumab and bevacizumab (hereafter referred to as "A-B") in cancer patients, and reduce future incidence of hypertension-related cardiovascular complications.
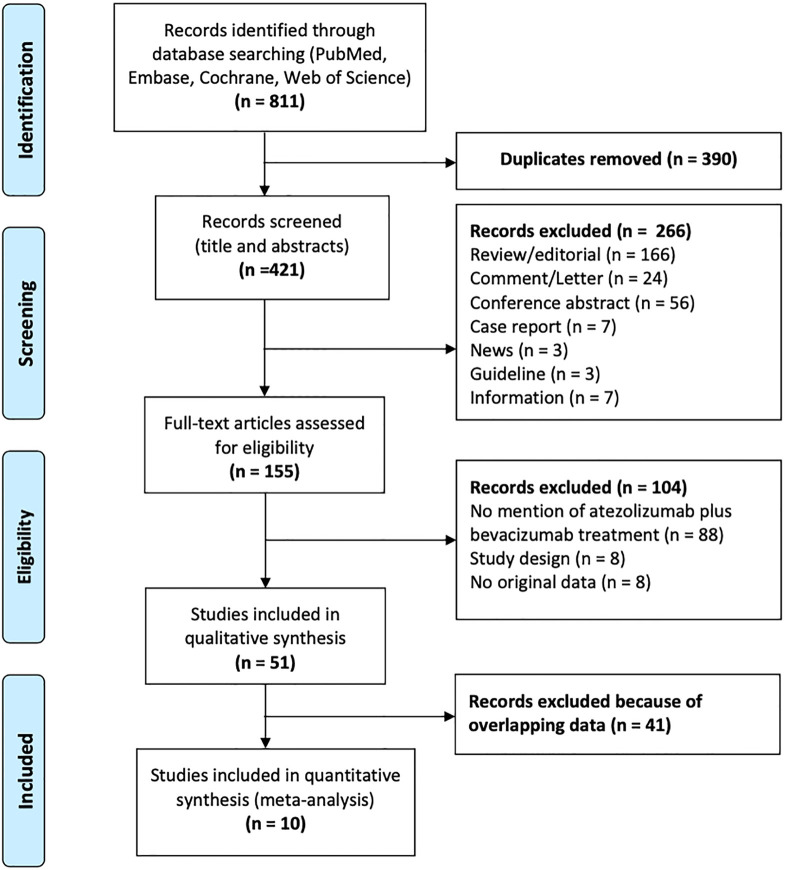
Databases, including PubMed, Embase, Cochrane, and Web of Science were searched to identify relevant studies, which were retrieved from inception to March 6, 2021. Studies focused on cancer patients treated with A-B that provided data on hypertension were included. Statistical analyses were conducted to calculate hypertension incidence and relative risk (RR) with a random-effects or fixed-effects model, hinging on heterogeneity status.
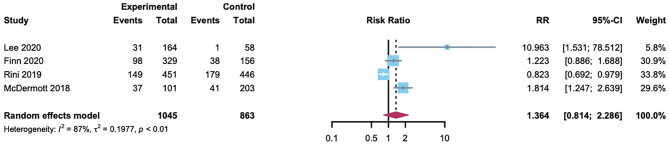
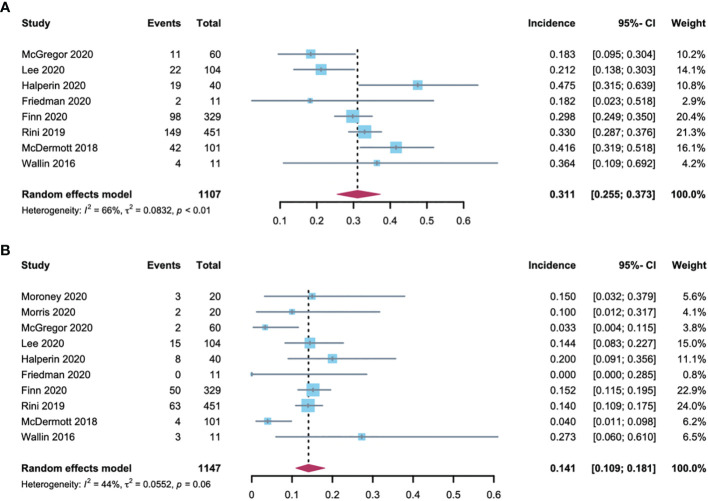
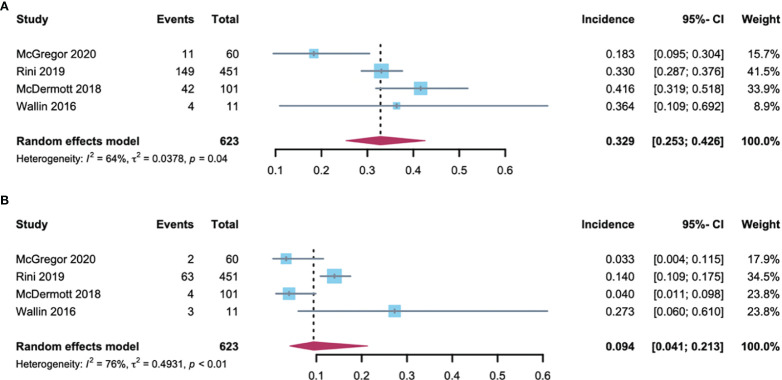
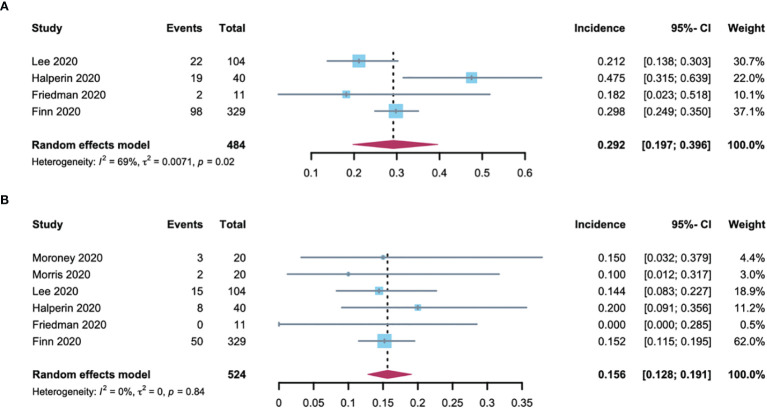
Ten studies including 2106 patients with renal cell carcinoma (RCC), hepatocellular carcinoma (HCC), ovarian cancer, anal cancer, neuroendocrine tumors (NETs), and cervical cancer were selected for this meta-analysis. For patients treated with A-B, the all-grade and high-grade (grade 3) hypertension incidence were 31.1% (95% CI: 25.5-37.3) and 14.1% (95% CI: 10.9-18.1), respectively. No significant difference was observed in all-grade hypertension incidence between RCC and a non-RCC patients (32.9% [95% CI: 25.3-42.6] 29.2% [95% CI: 19.7-39.6)]). However, the number of high-grade hypertension incidence in RCC patients (9.4% [95% CI: 4.1-21.3]) was lower than that of non-RCC patients (15.6% [95% CI: 12.8-19.1]). RCC or HCC patients who received the A-B treatment were associated with significantly increased risk of all-grade hypertension with a RR of 7.22 (95% CI: 3.3-15.7; = 0.6) compared with patients treated with atezolizumab.
Cancer Patients treated with atezolizumab and bevacizumab have a significantly increased risk of hypertension. Sufficient monitoring is highly recommended to prevent the consequences of treatment-induced hypertension and other cardiovascular complications.
本研究旨在为既往临床评估提供信息,以更好地了解癌症患者使用阿替利珠单抗和贝伐珠单抗(以下简称“A-B”)治疗时高血压的总体风险,并降低未来高血压相关心血管并发症的发生率。
检索包括PubMed、Embase、Cochrane和Web of Science在内的数据库,以识别相关研究,检索时间从数据库建立至2021年3月6日。纳入聚焦于接受A-B治疗且提供高血压数据的癌症患者的研究。根据异质性状态,采用随机效应或固定效应模型进行统计分析,以计算高血压发病率和相对风险(RR)。
本荟萃分析选取了10项研究,共2106例肾细胞癌(RCC)、肝细胞癌(HCC)、卵巢癌、肛门癌、神经内分泌肿瘤(NETs)和宫颈癌患者。接受A-B治疗的患者中,所有级别和高级别(3级)高血压发病率分别为31.1%(95%CI:25.5-37.3)和14.1%(95%CI:10.9-18.1)。RCC患者和非RCC患者的所有级别高血压发病率无显著差异(32.9%[95%CI:25.3-42.6]对29.2%[95%CI:19.7-39.6])。然而,RCC患者的高级别高血压发病率(9.4%[95%CI:4.1-21.3])低于非RCC患者(15.6%[95%CI:12.8-19.1])。与接受阿替利珠单抗治疗的患者相比,接受A-B治疗的RCC或HCC患者发生所有级别高血压的风险显著增加,RR为7.22(95%CI:3.3-15.7;I²=0.6)。
接受阿替利珠单抗和贝伐珠单抗治疗的癌症患者发生高血压的风险显著增加。强烈建议进行充分监测,以预防治疗引起的高血压及其他心血管并发症的后果。