Rauen Katrin, Vetter Stefan, Eisele Amanda, Biskup Ewelina, Delsignore Aba, Rufer Michael, Weidt Steffi
Department of Geriatric Psychiatry, Psychiatric Hospital Zurich, University of Zurich, Zurich, Switzerland.
Department of Psychiatry, Psychotherapy, and Psychosomatics, Psychiatric Hospital Zurich, University of Zurich, Zurich, Switzerland.
Front Digit Health. 2020 Jun 19;2:4. doi: 10.3389/fdgth.2020.00004. eCollection 2020.
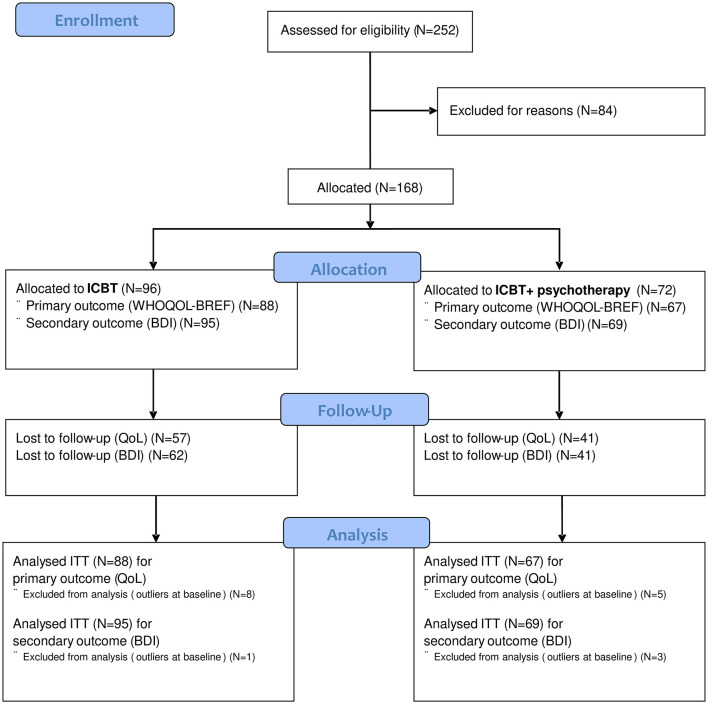
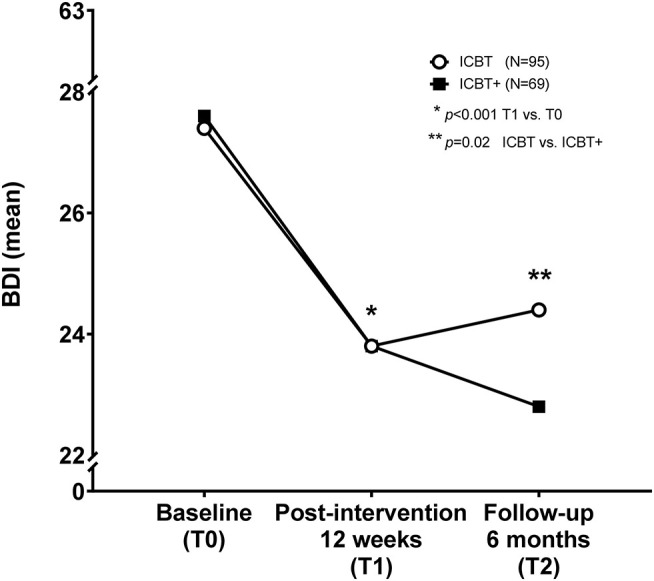
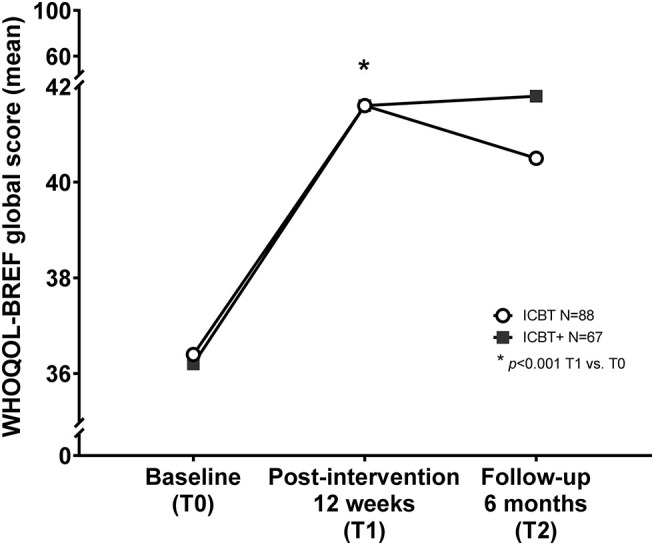
Depressive disorders are a curable, global health problem. However, most patients remain untreated, and more and more patients use internet-based interventions, but it is unclear whether it is beneficial for ongoing face-to-face psychotherapy. Thus, we compared the outcome of internet cognitive behavioral therapy (ICBT) with (ICBT+) or without (ICBT) additional face-to-face outpatient psychotherapy in adult patients with moderate to severe depressive disorder. For this longitudinal interventional clinical trial (NCT02112266), 168 of 252 online recruited adults with depressive symptoms received ICBT+ ( = 96) or ICBT ( = 72). Demographics (sex, age, age at first depressive episode, years of education, duration of depressive symptoms) were assessed and compared between groups. All patients underwent ICBT for 12 weeks. Quality of life (QoL) and severity of depressive symptoms were assessed within each group at three time points [baseline (T0), postinterventional after ICBT at 12 weeks (T1), and for follow-up at 6 months (T2)] using the World Health Organization Quality of Life Questionnaire (WHOQOL-BREF) global score to assess QoL as primary and the Beck Depression Inventory (BDI-II) to assess self-rated depressive symptoms as secondary outcome variables, respectively. Differences were assessed between groups using test and over time using repeated-measures analysis of variance. Data of intention-to-treat analysis are given as mean ± SD. Group differences were assumed at < 0.05. Partial η is given as effect size. Demographic data, QoL, and depressive symptoms did not differ between groups (ICBT+/ICBT) at baseline (T0). Patients of both groups suffered from moderate to severe depressive disorders and gained improved QoL scores (WHOQOL-BREF-global: < 0.001, η = 0.16), as well as experienced decreased depressive symptoms (BDI-II: < 0.001, η = 0.2) after 12 weeks of ICBT compared to baseline. Patients without additional face-to-face outpatient psychotherapy lost QoL-albeit not significant-and had increased depressive symptoms (BDI: = 0.02, η = 0.04) at 6 months' follow-up. Thus, ICBT is suitable for psychiatric treatment, although additional face-to-face outpatient psychotherapy helps stabilizing long-term outcome.
抑郁症是一个可治愈的全球性健康问题。然而,大多数患者仍未得到治疗,且越来越多的患者使用基于互联网的干预措施,但尚不清楚这对正在进行的面对面心理治疗是否有益。因此,我们比较了互联网认知行为疗法(ICBT)联合(ICBT +)或不联合(ICBT)额外面对面门诊心理治疗对中重度抑郁症成年患者的疗效。对于这项纵向干预性临床试验(NCT02112266),252名在线招募的有抑郁症状的成年人中,168人接受了ICBT +(n = 96)或ICBT(n = 72)。评估并比较了两组之间的人口统计学特征(性别、年龄、首次抑郁发作年龄、受教育年限、抑郁症状持续时间)。所有患者均接受了12周的ICBT治疗。在三个时间点[基线(T0)、ICBT治疗12周后的干预后(T1)以及6个月随访时(T2)],使用世界卫生组织生活质量问卷(WHOQOL - BREF)全球评分评估生活质量(QoL)作为主要结局变量,使用贝克抑郁量表(BDI - II)评估自评抑郁症状作为次要结局变量,对每组患者进行评估。使用t检验评估组间差异,并使用重复测量方差分析评估随时间的差异。意向性分析数据以均值±标准差表示。假设组间差异P < 0.05。部分η²作为效应量给出。在基线(T0)时,两组(ICBT + / ICBT)之间的人口统计学数据、生活质量和抑郁症状无差异。两组患者均患有中重度抑郁症,与基线相比,经过12周的ICBT治疗后,生活质量评分得到改善(WHOQOL - BREF全球评分:P < 0.001,η² = 0.16),抑郁症状也有所减轻(BDI - II:P < 0.001,η² = 0.2)。在6个月随访时,未接受额外面对面门诊心理治疗的患者生活质量有所下降(尽管不显著),抑郁症状有所增加(BDI:P = 0.02,η² = 0.04)。因此,ICBT适用于精神疾病治疗,尽管额外的面对面门诊心理治疗有助于稳定长期疗效。