National Clinician Scholars Program, University of Michigan, Ann Arbor.
Department of General Surgery, Stanford University, Stanford, California.
JAMA Netw Open. 2021 Oct 1;4(10):e2132103. doi: 10.1001/jamanetworkopen.2021.32103.
Financial hardship affects health care access and health outcomes among peripartum women.
To evaluate the prevalence of financial hardship among peripartum women over time and by insurance type and income.
DESIGN, SETTING, AND PARTICIPANTS: This cross-sectional study included peripartum women, defined as women aged 18 to 45 years who reported being currently pregnant or pregnant in the past 12 months, who participated in the National Health Interview Survey from 2013 to 2018. Data were analyzed from January to May 2021.
Current pregnancy or recent pregnancy as well as insurance type and income.
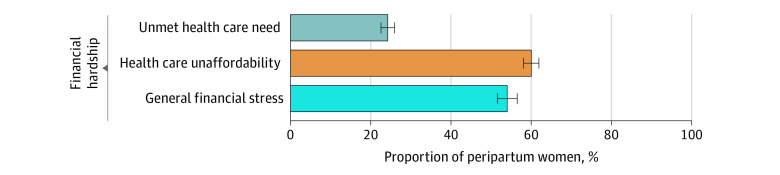
Three measures of financial hardship within the last year were evaluated: (1) unmet health care need due to cost (unmet need for medical care or delayed or deferred medical care due to cost); (2) health care unaffordability (worry about paying for potential medical bills or existing medical debt); and (3) general financial stress (worry about subsistence spending [eg, monthly bills, housing]).
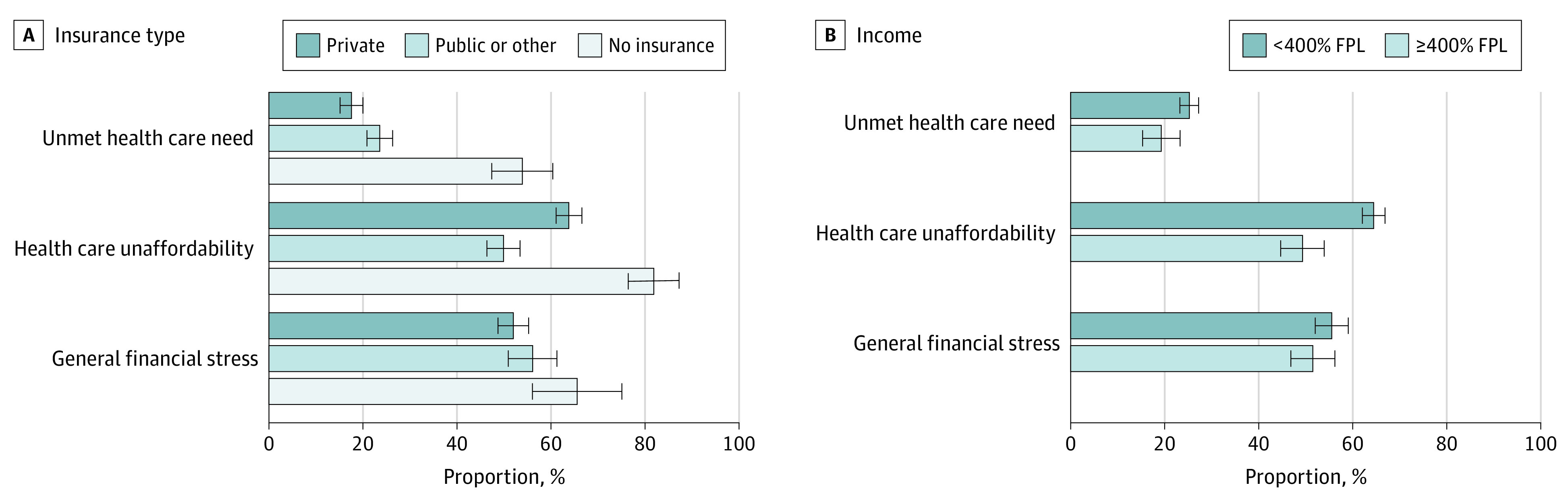
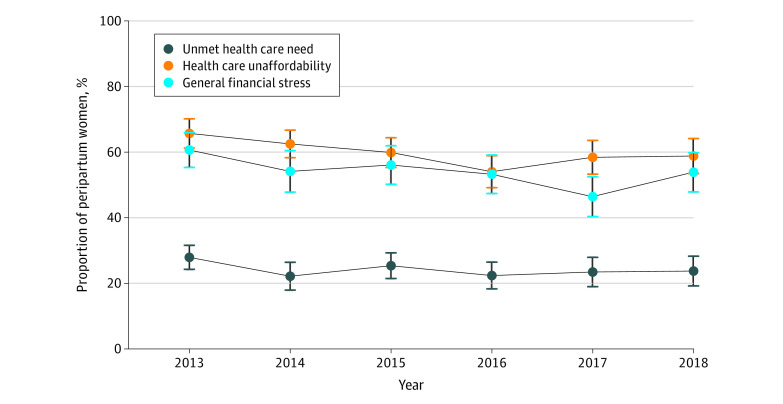
The study cohort included 3509 peripartum women, weighted to represent 1 050 789 women (2018: an estimated 36 045 of 184 018 [19.6%] Hispanic, 39 017 [21.2%] Black, and 97 366 [52.9%] White), with a mean (SD) age of 29 (6) years. Overall, from 2013 to 2018, 24.2% (95% CI, 22.6%-26.0%) of peripartum women reported unmet health care need, 60.0% (95% CI, 58.0%-61.9%) reported health care unaffordability, and 54.0% (95% CI, 51.5%-56.5%) reported general financial stress. The prevalence of financial hardship outcomes did not substantially change between 2013 and 2018 (unmet health care need in 2013: 27.9% [95% CI, 24.4%-31.7%]; in 2018: 23.7% [95% CI, 19.5%-28.6%]; health care unaffordability in 2013: 65.7% [95% CI, 61.1%-70.0%]; in 2018: 58.8% [95% CI, 53.4%-64.0%]; general financial stress in 2013: 60.6% [95% CI, 55.2%-65.8%]; in 2018: 53.8% [95% CI, 47.8%-59.8%]). Women with private insurance had lower odds of unmet need (adjusted odds ratio [aOR], 0.67; 95% CI, 0.52-0.87) but higher odds of health care unaffordability (aOR, 1.88; 95% CI, 1.49-2.36) compared with women with public insurance. Peripartum women with household incomes less than 400% of the federal poverty level had higher odds of unmet need (aOR, 1.50; 95% CI, 1.08-2.08) and unaffordable care (aOR, 1.98; 95% CI, 1.54-2.55) compared with those with household incomes 400% or more of federal poverty level.
These findings suggest that financial hardship among peripartum women in the United States was common from 2013 to 2018, including 24% of pregnant and postpartum women reporting unmet health care need and 60% reporting health care unaffordability. Women with private insurance and those living on lower incomes were more likely to experience unaffordable health care than women with pubic insurance and those with higher incomes, respectively. Targeted policy interventions are needed to improve health care affordability and promote overall economic security among peripartum women.
经济困难会影响围产期妇女获得医疗保健的机会和健康结果。
评估一段时间内不同保险类型和收入的围产期妇女经济困难的发生率。
设计、地点和参与者:本横断面研究纳入了年龄在 18 至 45 岁之间的目前怀孕或过去 12 个月内怀孕的围产期妇女,她们参加了 2013 年至 2018 年的全国健康访谈调查。数据分析于 2021 年 1 月至 5 月进行。
目前怀孕或最近怀孕,以及保险类型和收入。
评估了过去一年中三种经济困难的指标:(1)因费用而无法获得医疗服务的需求(因费用而无法获得医疗服务或延迟或推迟医疗服务);(2)医疗服务负担能力(担心支付潜在的医疗费用或现有的医疗债务);(3)一般经济压力(担心维持生计的支出[例如,每月账单、住房])。
研究队列包括 3509 名围产期妇女,经加权后代表 1050789 名妇女(2018 年:估计有 184018 名中的 36045 名是西班牙裔[19.6%],39017 名是黑人[21.2%],97366 名是白人[52.9%]),平均年龄(标准差)为 29(6)岁。总体而言,从 2013 年到 2018 年,24.2%(95%置信区间,22.6%-26.0%)的围产期妇女报告存在未满足的医疗服务需求,60.0%(95%置信区间,58.0%-61.9%)报告医疗服务负担能力不足,54.0%(95%置信区间,51.5%-56.5%)报告一般经济压力。2013 年至 2018 年期间,经济困难结果的发生率没有明显变化(2013 年未满足的医疗服务需求:27.9%[95%置信区间,24.4%-31.7%];2018 年:23.7%[95%置信区间,19.5%-28.6%];医疗服务负担能力不足 2013 年:65.7%[95%置信区间,61.1%-70.0%];2018 年:58.8%[95%置信区间,53.4%-64.0%];一般经济压力 2013 年:60.6%[95%置信区间,55.2%-65.8%];2018 年:53.8%[95%置信区间,47.8%-59.8%])。与拥有公共保险的妇女相比,拥有私人保险的妇女未满足需求的可能性较小(调整后的优势比[aOR],0.67;95%置信区间,0.52-0.87),但无法负担医疗保健的可能性较大(aOR,1.88;95%置信区间,1.49-2.36)。家庭收入低于联邦贫困水平 400%的围产期妇女与收入 400%或以上的家庭相比,未满足需求的可能性更高(aOR,1.50;95%置信区间,1.08-2.08),无法负担医疗保健的可能性也更高(aOR,1.98;95%置信区间,1.54-2.55)。
这些发现表明,2013 年至 2018 年期间,美国围产期妇女的经济困难较为普遍,包括 24%的孕妇和产后妇女报告存在未满足的医疗服务需求,60%的妇女报告存在无法负担的医疗保健。与拥有公共保险和高收入的妇女相比,拥有私人保险和低收入的妇女更有可能面临无法负担的医疗保健。需要采取有针对性的政策干预措施,以提高医疗保健的可负担性,促进围产期妇女的整体经济安全。