Division of Respiratory Medicine, Department of Internal Medicine, Kobe University Graduate School of Medicine, Kobe, Japan.
Department of Diagnostic Pathology, Kobe University Graduate School of Medicine, Kobe, Japan.
PLoS One. 2021 Oct 29;16(10):e0259236. doi: 10.1371/journal.pone.0259236. eCollection 2021.
Adequate tumor tissue is required to make the best treatment choice for non-small cell lung cancer (NSCLC). Transbronchial biopsy (TBB) by endobronchial ultrasonography with a guide sheath (EBUS-GS) is useful to diagnose peripheral lung lesions. The data of tumor cell numbers obtained by two different sizes of GSs is limited. We conducted this study to investigate the utility of a large GS kit to obtain many tumor cells in patients with NSCLC.
Patients with a peripheral lung lesion and suspected of NSCLC were prospectively enrolled. They underwent TBB with a 5.9-mm diameter bronchoscope with a large GS. When the lesion was invisible in EBUS, we changed to a thinner bronchoscope and TBB was performed with a small GS. We compared the tumor cell number prospectively obtained with a large GS (prospective large GS group) and those previously obtained with a small GS (small GS cohort). The primary endpoint was the tumor cell number per sample, and we assessed characteristics of lesions that could be obtained by TBB with large GS.
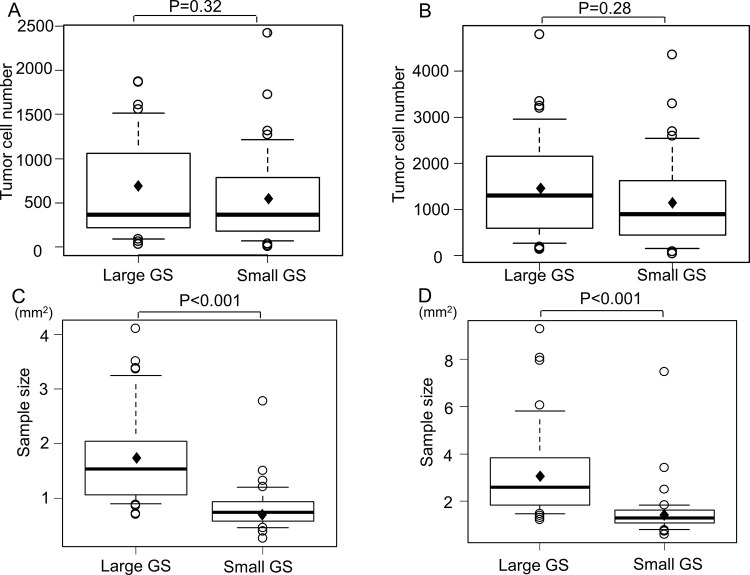
Biopsy with large GS was performed in 55 of 87 patients (63.2%), and 37 were diagnosed with NSCLC based on histological samples. The number of tumor cells per sample was not different between two groups (658±553 vs. 532±526, estimated difference between two groups with 95% confidence interval (CI); 125 (-125-376), p = 0.32). The sample size of the large GS group was significantly larger than that of the small GS cohort (1.75 mm2 vs. 0.83 mm2, estimated difference with 95% CI; 0.92 (0.60-1.23) mm2, p = 0.00000019). The lesion involving a third or less bronchus generation was predictive factors using large GS.
The sample size obtained with large GS was significantly larger compared to that obtained with small GS, but there was no significant difference in tumor cell number. The 5.9-mm diameter bronchoscope with large GS can be used for lesions involving a third or less bronchus generation.
非小细胞肺癌 (NSCLC) 需要足够的肿瘤组织来做出最佳治疗选择。经支气管内超声引导下的支气管镜活检术(EBUS-GS)对于诊断周围性肺病变很有用。通过两种不同大小的 GS 获得的肿瘤细胞数量数据有限。我们进行这项研究,旨在探讨使用大 GS 套件从 NSCLC 患者中获得大量肿瘤细胞的效用。
前瞻性纳入外周肺病变且疑似 NSCLC 的患者。他们接受了 5.9 毫米直径支气管镜和大 GS 的 TBB。当 EBUS 中看不见病变时,我们改用更细的支气管镜,并用小 GS 进行 TBB。我们前瞻性比较了大 GS 获得的肿瘤细胞数量(前瞻性大 GS 组)和以前用小 GS 获得的细胞数量(小 GS 队列)。主要终点是每个样本的肿瘤细胞数量,我们评估了可以用大 GS 进行 TBB 的病变的特征。
55 例患者(63.2%)进行了大 GS 活检,37 例患者根据组织学样本诊断为 NSCLC。两组间样本中的肿瘤细胞数量无差异(658±553 与 532±526,两组间差异的估计值,95%置信区间 (CI);125 (-125-376),p = 0.32)。大 GS 组的样本量明显大于小 GS 队列(1.75 毫米 2 与 0.83 毫米 2,大 GS 组样本量的估计值,95%CI;0.92(0.60-1.23)毫米 2,p = 0.00000019)。涉及三级或三级以下支气管生成的病变是使用大 GS 的预测因素。
与小 GS 相比,大 GS 获得的样本量明显更大,但肿瘤细胞数量无显著差异。5.9 毫米直径的支气管镜和大 GS 可用于涉及三级或三级以下支气管生成的病变。