Moskowitz Ari, Berg Katherine M, Cocchi Michael N, Grossestreuer Anne V, Issa Mahmoud, Balaji Lakshman, Chase Maureen, Yang Jesse X, Sarge Jennifer, O'Donoghue Sharon, Sarge Todd, Donnino Michael W
Center for Resuscitation Science, Beth Israel Deaconess Medical Center, Boston, MA.
Division of Pulmonary, Critical Care, and Sleep Medicine, Beth Israel Deaconess Medical Center, Boston, MA.
Crit Care Explor. 2021 Oct 18;3(10):e0557. doi: 10.1097/CCE.0000000000000557. eCollection 2021 Oct.
Although patients in the ICU are closely monitored, some ICU cardiac arrest events may be preventable. In this study, we sought to reduce the rate of cardiac arrests occurring in the ICU through a quality improvement initiative.
Prospective, observational study.
ICUs of a single tertiary care center.
Patients hospitalized in the ICUs between August 2017 and November 2019.
A comprehensive trigger and response tool.
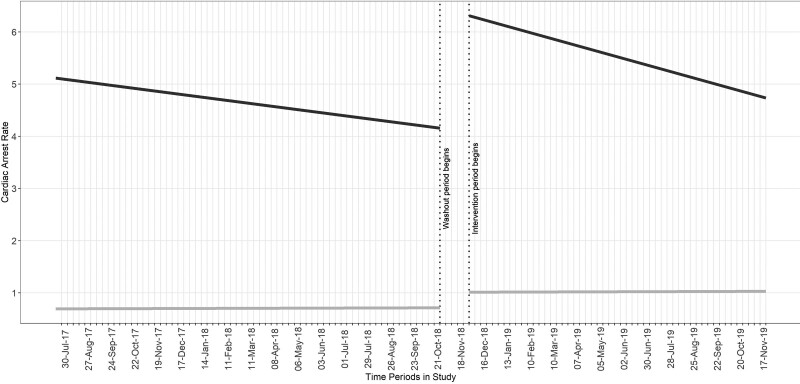
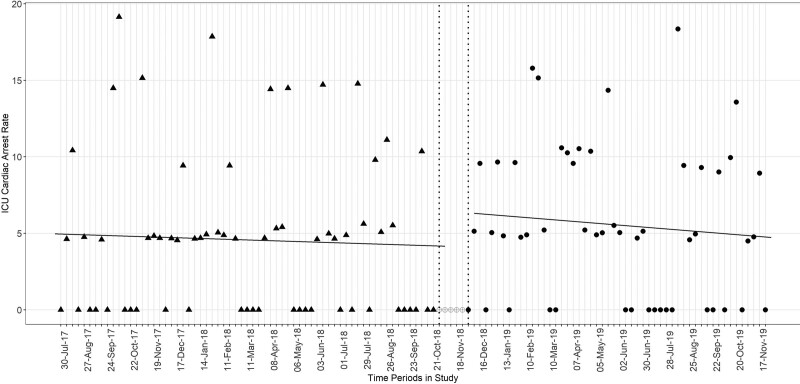
Forty-three patients experienced an ICU cardiac arrest in the preintervention epoch (6.79 arrests per 1,000 discharges), and 59 patients experienced an ICU cardiac arrest in the intervention epoch (7.91 arrests per 1,000 discharges). In the intervention epoch, the clinical trigger and response tool was activated 106 times over a 1-year period, most commonly due to unexpected new/worsening hypotension. There was no step change in arrest rate (2.24 arrests/1,000 patients; 95% CI, -1.82 to 6.28; = 0.28) or slope change (-0.02 slope of arrest rate; 95% CI, -0.14 to 0.11; = 0.79) comparing the preintervention and intervention time epochs. Cardiac arrests in the preintervention epoch were more likely to be "potentially preventable" than that in the intervention epoch (25.6% vs 12.3%, respectively; odds ratio, 0.58; 95% CI, 0.20-0.88; < 0.01).
A novel trigger-and-response tool did not reduce the frequency of ICU cardiac arrest. Additional investigation is needed into the optimal approach for ICU cardiac arrest prevention.
尽管重症监护病房(ICU)的患者受到密切监测,但一些ICU心脏骤停事件可能是可以预防的。在本研究中,我们试图通过一项质量改进措施来降低ICU中发生心脏骤停的比率。
前瞻性观察性研究。
一家三级医疗中心的ICU。
2017年8月至2019年11月期间在ICU住院的患者。
一种综合触发和应对工具。
在干预前阶段,43名患者发生了ICU心脏骤停(每1000例出院患者中有6.79次心脏骤停),在干预阶段,59名患者发生了ICU心脏骤停(每1000例出院患者中有7.91次心脏骤停)。在干预阶段,临床触发和应对工具在1年时间内被激活106次,最常见的原因是意外的新出现/加重的低血压。比较干预前和干预阶段,心脏骤停发生率没有阶跃变化(2.24次心脏骤停/1000例患者;95%置信区间,-1.82至6.28;P = 0.28),心脏骤停发生率斜率也没有变化(心脏骤停发生率斜率为-0.02;95%置信区间,-0.14至0.11;P = 0.79)。干预前阶段的心脏骤停比干预阶段更有可能是“潜在可预防的”(分别为25.6%和12.3%;优势比,0.58;95%置信区间,0.20 - 0.88;P < 0.01)。
一种新型的触发和应对工具并未降低ICU心脏骤停的频率。需要对预防ICU心脏骤停的最佳方法进行进一步研究。