Division of Pulmonary, Allergy, and Critical Care Medicine, Duke University, Durham, NC.
Division of Infectious Disease, Duke University, Durham, NC.
Crit Care Med. 2019 Jan;47(1):49-55. doi: 10.1097/CCM.0000000000003439.
Previous studies have looked at National Early Warning Score performance in predicting in-hospital deterioration and death, but data are lacking with respect to patient outcomes following implementation of National Early Warning Score. We sought to determine the effectiveness of National Early Warning Score implementation on predicting and preventing patient deterioration in a clinical setting.
Retrospective cohort study.
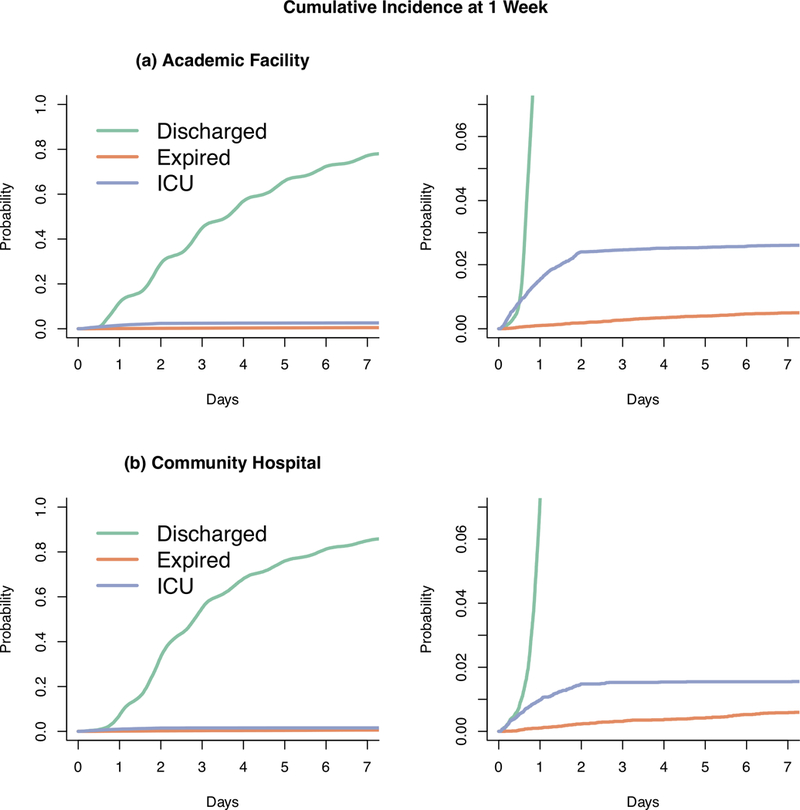
Tertiary care academic facility and a community hospital.
Patients 18 years old or older hospitalized from March 1, 2014, to February 28, 2015, during preimplementation of National Early Warning Score to August 1, 2015, to July 31, 2016, after National Early Warning Score was implemented.
Implementation of National Early Warning Score within the electronic health record and associated best practice alert.
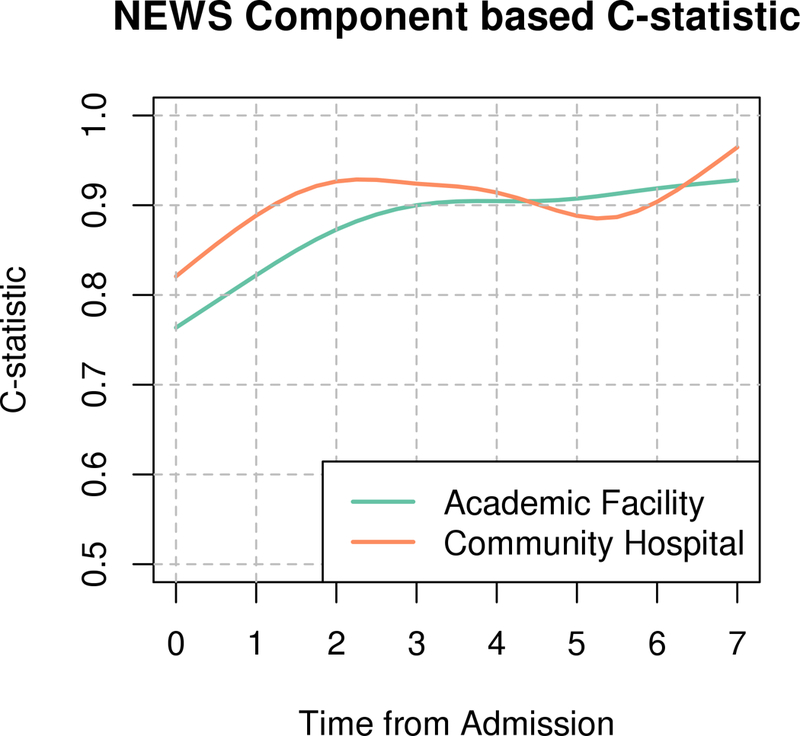
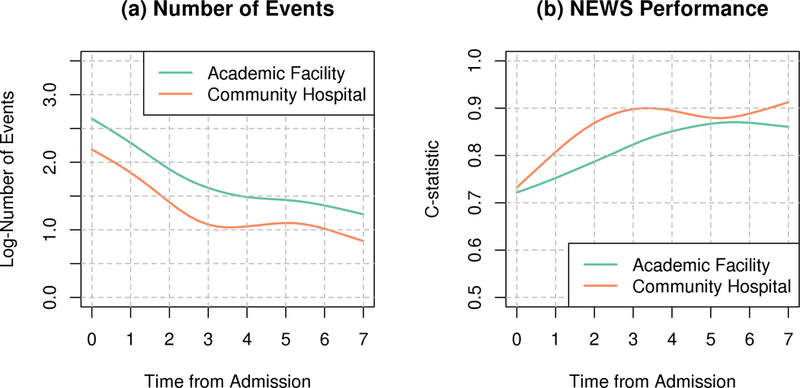
In this study of 85,322 patients (42,402 patients pre-National Early Warning Score and 42,920 patients post-National Early Warning Score implementation), the primary outcome of rate of ICU transfer or death did not change after National Early Warning Score implementation, with adjusted hazard ratio of 0.94 (0.84-1.05) and 0.90 (0.77-1.05) at our academic and community hospital, respectively. In total, 175,357 best practice advisories fired during the study period, with the best practice advisory performing better at the community hospital than the academic at predicting an event within 12 hours 7.4% versus 2.2% of the time, respectively. Retraining National Early Warning Score with newly generated hospital-specific coefficients improved model performance.
At both our academic and community hospital, National Early Warning Score had poor performance characteristics and was generally ignored by frontline nursing staff. As a result, National Early Warning Score implementation had no appreciable impact on defined clinical outcomes. Refitting of the model using site-specific data improved performance and supports validating predictive models on local data.
先前的研究已经探讨了国家早期预警评分在预测住院患者恶化和死亡方面的性能,但在实施国家早期预警评分后,关于患者预后的数据却很缺乏。我们试图确定在临床环境中实施国家早期预警评分对预测和预防患者恶化的有效性。
回顾性队列研究。
三级保健学术机构和社区医院。
2014 年 3 月 1 日至 2015 年 2 月 28 日期间在实施国家早期预警评分前,以及 2015 年 8 月 1 日至 2016 年 7 月 31 日期间在实施国家早期预警评分后,年龄在 18 岁或以上住院的患者。
在电子健康记录中实施国家早期预警评分和相关最佳实践警报。
在这项涉及 85322 名患者的研究中(实施国家早期预警评分前 42402 名患者,实施国家早期预警评分后 42920 名患者),在 ICU 转科或死亡的主要结局方面,在实施国家早期预警评分后并没有改变,调整后的危险比分别为 0.94(0.84-1.05)和 0.90(0.77-1.05),在我们的学术和社区医院。在研究期间,共发出了 175357 次最佳实践建议,社区医院的最佳实践建议在 12 小时内预测事件的性能优于学术医院,分别为 7.4%和 2.2%。使用新生成的特定于医院的系数重新训练国家早期预警评分可提高模型性能。
在我们的学术和社区医院,国家早期预警评分的性能特征都较差,并且通常被一线护理人员忽视。因此,实施国家早期预警评分对确定的临床结果没有明显影响。使用特定于站点的数据重新拟合模型提高了性能,并支持在本地数据上验证预测模型。