Guo Rong-Jing, Gao Ting, Ruan Zhe, Zhou Hong-Yu, Gao Feng, Xu Quan, Yu Li-Ping, Wu Song-Di, Lei Tao, Li Huan-Huan, Sun Chao, Zhang Min, Gao Yan-Wu, Lu Xiao-Dan, Tang Yong-Lan, Tang Bao-Li, Huo Fei-Yan, Zhu Ying, Li Zhu-Yi, Chang Ting
Department of Neurology, Tangdu Hospital, The Fourth Military Medical University, Xi'an, 710038, China.
Department of Neurology, West China Hospital, Sichuan University, Chengdu, China.
Neurol Ther. 2022 Mar;11(1):73-86. doi: 10.1007/s40120-021-00292-x. Epub 2021 Nov 2.
Many patients with ocular myasthenia gravis (OMG) progress to generalized disease within the first 2 years of the onset of ocular symptoms. Several retrospective studies have identified risk factors associated with generalization, however these studies included patients on immunosuppression therapy or those undergoing thymectomy, which may reduce the generalization risk. In this study we explored the risk factors for generalization in non-immunosuppressed and non-thymectomized patients with OMG.
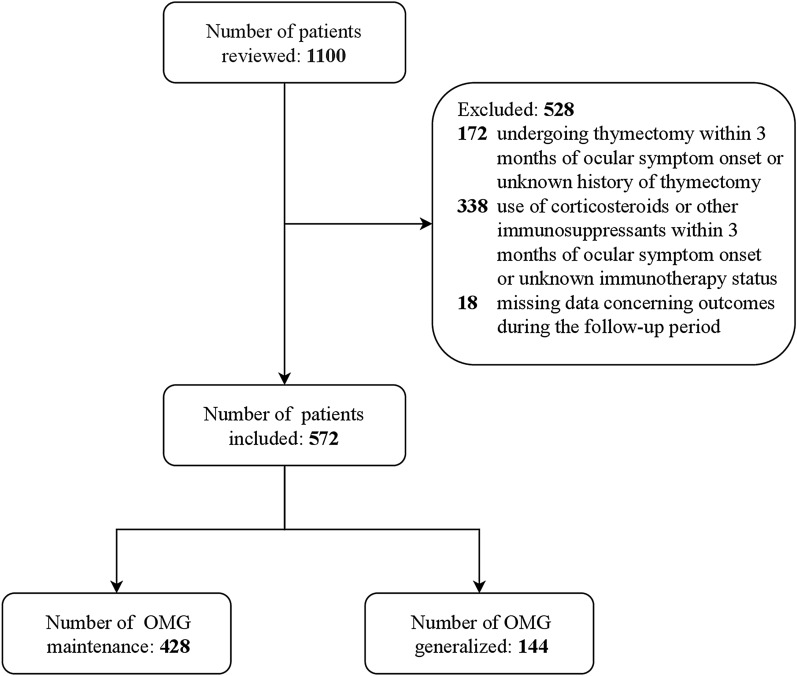
Data from patients with OMG treated at seven tertiary hospitals in China were retrospectively reviewed. Clinical characteristics, including sex, age at onset, symptoms at onset, comorbid autoimmune diseases, neostigmine test response, repetitive nerve stimulation (RNS) findings, presence of serum anti-acetylcholine receptor antibody (AChR-Ab), and thymic status based on radiological and pathological studies, were collected. The main outcome measure was disease generalization. The follow-up period was defined as the date of ocular symptom onset to the date of confirmation of generalization or immunotherapy initiation, or last follow-up (defined as 60 months). The Cox proportional hazards model was used to assess the risk factors for generalization.
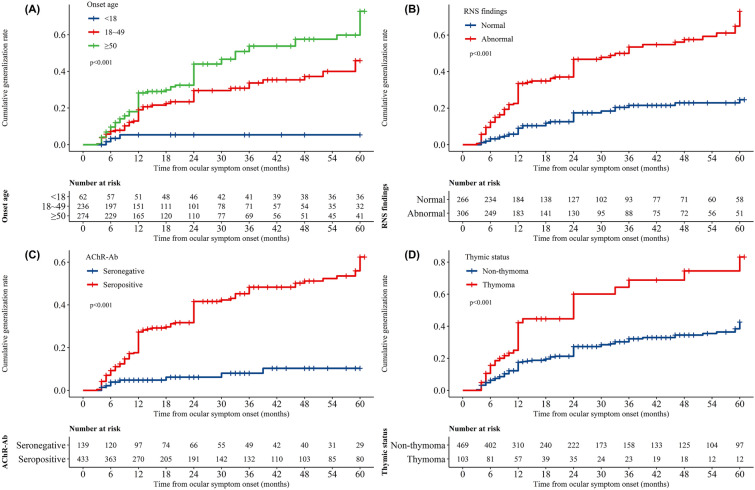
Overall, 572 patients (269 women) were eligible for inclusion in the analysis, of whom 144 developed generalization. The mean (standard deviation) onset age was 45.5 (19.8) years, and the median (interquartile range) follow-up period was 14.5 (7.0-47.3) months. Multivariable Cox regression analysis demonstrated that both early-onset (adjusted hazard ratio [aHR] 5.34; 95% confidence interval [CI] 1.64-17.36; p = 0.005) and late-onset (aHR 7.18; 95% CI 2.22-23.27; p = 0.001) in adulthood, abnormal RNS findings (aHR 3.01; 95% CI 1.97-4.61; p < 0.001), seropositivity for AChR-Ab (aHR 2.58; 95% CI 1.26-5.26; p = 0.01), and thymoma (aHR 1.62; 95% CI 1.05-2.49; p = 0.03) were independently associated with increased risk of generalization.
The risk of generalization increased significantly in patients with adult-onset OMG, abnormal RNS findings, seropositivity for AChR-Ab, and thymoma, suggesting that these risk factors may predict OMG generalization.
许多眼肌型重症肌无力(OMG)患者在出现眼部症状的头2年内病情进展为全身型疾病。多项回顾性研究已确定了与病情进展相关的危险因素,然而这些研究纳入了接受免疫抑制治疗的患者或接受胸腺切除术的患者,这可能降低了病情进展的风险。在本研究中,我们探讨了未接受免疫抑制治疗且未接受胸腺切除术的OMG患者病情进展的危险因素。
回顾性分析中国7家三级医院收治的OMG患者的数据。收集临床特征,包括性别、发病年龄、起病症状、合并的自身免疫性疾病、新斯的明试验反应、重复神经电刺激(RNS)结果、血清抗乙酰胆碱受体抗体(AChR-Ab)的存在情况以及基于影像学和病理学研究的胸腺状态。主要观察指标为疾病进展。随访期定义为眼部症状出现之日至病情进展确认或免疫治疗开始之日,或最后一次随访(定义为60个月)。采用Cox比例风险模型评估病情进展的危险因素。
总体而言,572例患者(269例女性)符合纳入分析的条件,其中144例病情进展。平均(标准差)发病年龄为45.5(19.8)岁,中位(四分位间距)随访期为14.5(7.0 - 47.3)个月。多变量Cox回归分析表明,成年期早发(调整后风险比[aHR] 5.34;95%置信区间[CI] 1.64 - 17.36;p = 0.005)和晚发(aHR 7.18;95% CI 2.22 - 23.27;p = 0.001)、RNS结果异常(aHR 3.01;95% CI 1.97 - 4.61;p < 0.001)、AChR-Ab血清学阳性(aHR 2.58;95% CI 1.26 - 5.26;p = 0.01)以及胸腺瘤(aHR 1.62;95% CI 1.05 - 2.49;p = 0.03)均与病情进展风险增加独立相关。
成年期发病的OMG患者、RNS结果异常、AChR-Ab血清学阳性以及胸腺瘤患者病情进展的风险显著增加,提示这些危险因素可能预测OMG病情进展。