Mitra Avijit, Ahsan Hiba, Li Wenjun, Liu Weisong, Kerns Robert D, Tsai Jack, Becker William, Smelson David A, Yu Hong
College of Information and Computer Sciences, University of Massachusetts Amherst, Amherst, MA, United States.
Department of Public Health, University of Massachusetts Lowell, Lowell, MA, United States.
JMIR Med Inform. 2021 Nov 8;9(11):e32851. doi: 10.2196/32851.
Opioid overdose (OD) and related deaths have significantly increased in the United States over the last 2 decades. Existing studies have mostly focused on demographic and clinical risk factors in noncritical care settings. Social and behavioral determinants of health (SBDH) are infrequently coded in the electronic health record (EHR) and usually buried in unstructured EHR notes, reflecting possible gaps in clinical care and observational research. Therefore, SBDH often receive less attention despite being important risk factors for OD. Natural language processing (NLP) can alleviate this problem.
The objectives of this study were two-fold: First, we examined the usefulness of NLP for SBDH extraction from unstructured EHR text, and second, for intensive care unit (ICU) admissions, we investigated risk factors including SBDH for nonfatal OD.
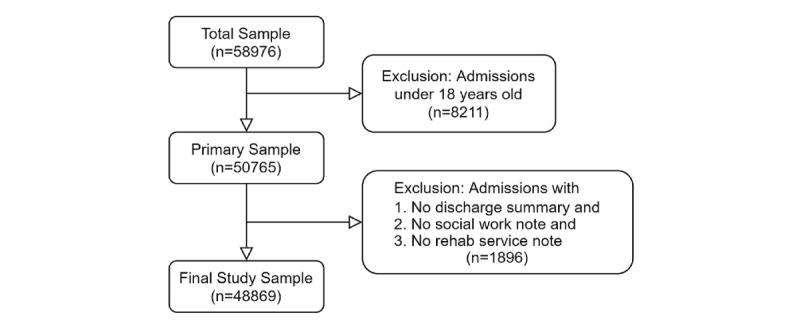
We performed a cross-sectional analysis of admission data from the EHR of patients in the ICU of Beth Israel Deaconess Medical Center between 2001 and 2012. We used patient admission data and International Classification of Diseases, Ninth Revision (ICD-9) diagnoses to extract demographics, nonfatal OD, SBDH, and other clinical variables. In addition to obtaining SBDH information from the ICD codes, an NLP model was developed to extract 6 SBDH variables from EHR notes, namely, housing insecurity, unemployment, social isolation, alcohol use, smoking, and illicit drug use. We adopted a sequential forward selection process to select relevant clinical variables. Multivariable logistic regression analysis was used to evaluate the associations with nonfatal OD, and relative risks were quantified as covariate-adjusted odds ratios (aOR).
The strongest association with nonfatal OD was found to be drug use disorder (aOR 8.17, 95% CI 5.44-12.27), followed by bipolar disorder (aOR 2.69, 95% CI 1.68-4.29). Among others, major depressive disorder (aOR 2.57, 95% CI 1.12-5.88), being on a Medicaid health insurance program (aOR 2.26, 95% CI 1.43-3.58), history of illicit drug use (aOR 2.09, 95% CI 1.15-3.79), and current use of illicit drugs (aOR 2.06, 95% CI 1.20-3.55) were strongly associated with increased risk of nonfatal OD. Conversely, Blacks (aOR 0.51, 95% CI 0.28-0.94), older age groups (40-64 years: aOR 0.65, 95% CI 0.44-0.96; >64 years: aOR 0.16, 95% CI 0.08-0.34) and those with tobacco use disorder (aOR 0.53, 95% CI 0.32-0.89) or alcohol use disorder (aOR 0.64, 95% CI 0.42-1.00) had decreased risk of nonfatal OD. Moreover, 99.82% of all SBDH information was identified by the NLP model, in contrast to only 0.18% identified by the ICD codes.
This is the first study to analyze the risk factors for nonfatal OD in an ICU setting using NLP-extracted SBDH from EHR notes. We found several risk factors associated with nonfatal OD including SBDH. SBDH are richly described in EHR notes, supporting the importance of integrating NLP-derived SBDH into OD risk assessment. More studies in ICU settings can help health care systems better understand and respond to the opioid epidemic.
在过去20年中,美国阿片类药物过量(OD)及相关死亡人数显著增加。现有研究大多集中在非重症监护环境中的人口统计学和临床风险因素。健康的社会和行为决定因素(SBDH)在电子健康记录(EHR)中很少被编码,通常隐藏在非结构化的EHR记录中,这反映出临床护理和观察性研究可能存在差距。因此,尽管SBDH是OD的重要风险因素,但往往较少受到关注。自然语言处理(NLP)可以缓解这一问题。
本研究的目的有两个:第一,我们检验了NLP从非结构化EHR文本中提取SBDH的有用性;第二,对于重症监护病房(ICU)入院患者,我们调查了包括SBDH在内的非致命OD的风险因素。
我们对2001年至2012年贝斯以色列女执事医疗中心ICU患者的EHR入院数据进行了横断面分析。我们使用患者入院数据和国际疾病分类第九版(ICD-9)诊断来提取人口统计学信息、非致命OD、SBDH和其他临床变量。除了从ICD编码中获取SBDH信息外,还开发了一个NLP模型,从EHR记录中提取6个SBDH变量,即住房不安全、失业、社会隔离、饮酒、吸烟和非法药物使用。我们采用逐步向前选择过程来选择相关的临床变量。多变量逻辑回归分析用于评估与非致命OD的关联,相对风险量化为协变量调整比值比(aOR)。
发现与非致命OD关联最强的是药物使用障碍(aOR 8.17,95%CI 5.44-12.27),其次是双相情感障碍(aOR 2.69,95%CI 1.68-4.29)。此外,重度抑郁症(aOR 2.57,95%CI 1.12-5.88)、参加医疗补助医疗保险计划(aOR 2.26,95%CI 1.43-3.58)、非法药物使用史(aOR 2.09,95%CI 1.15-3.79)和当前非法药物使用(aOR 2.06, 95%CI 1.20-3.55)与非致命OD风险增加密切相关。相反,黑人(aOR 0.51,95%CI 0.28-0.94)、老年人群(40-64岁:aOR 0.65,95%CI 0.44-0.96;>64岁:aOR 0.16,95%CI 0.08-0.34)以及患有烟草使用障碍(aOR 0.53,95%CI 0.32-0.89)或酒精使用障碍(aOR 0.64,95%CI 0.42-1.00)的人非致命OD风险降低。此外,所有SBDH信息的(99.82%)由NLP模型识别,相比之下,ICD编码仅识别了(0.18%)。
这是第一项使用从EHR记录中通过NLP提取的SBDH分析ICU环境中非致命OD风险因素的研究。我们发现了几个与非致命OD相关的风险因素,包括SBDH。EHR记录中对SBDH有丰富的描述,支持将NLP衍生的SBDH纳入OD风险评估的重要性。在ICU环境中进行更多研究有助于医疗保健系统更好地理解和应对阿片类药物流行。