Department of Emergency Medicine, University of Occupational and Environmental Health, 1-1 Iseigaoka, Yahata-nishi, Kitakyushu, 807-8555, Japan.
Department of Emergency and Critical Care Medicine, Chiba University Graduate School of Medicine, Chiba, Japan.
BMC Emerg Med. 2021 Nov 8;21(1):132. doi: 10.1186/s12873-021-00534-z.
Shock and organ damage occur in critically ill patients in the emergency department because of biological responses to invasion, and cytokines play an important role in their development. It is important to predict early multiple organ dysfunction (MOD) because it is useful in predicting patient outcomes and selecting treatment strategies. This study examined the accuracy of biomarkers, including interleukin (IL)-6, in predicting early MOD in critically ill patients compared with that of quick sequential organ failure assessment (qSOFA).
This was a multicenter observational sub-study. Five universities from 2016 to 2018. Data of adult patients with systemic inflammatory response syndrome who presented to the emergency department or were admitted to the intensive care unit were prospectively evaluated. qSOFA score and each biomarker (IL-6, IL-8, IL-10, tumor necrosis factor-α, C-reactive protein, and procalcitonin [PCT]) level were assessed on Days 0, 1, and 2. The primary outcome was set as MOD on Day 2, and the area under the curve (AUC) was analyzed to evaluate qSOFA scores and biomarker levels.
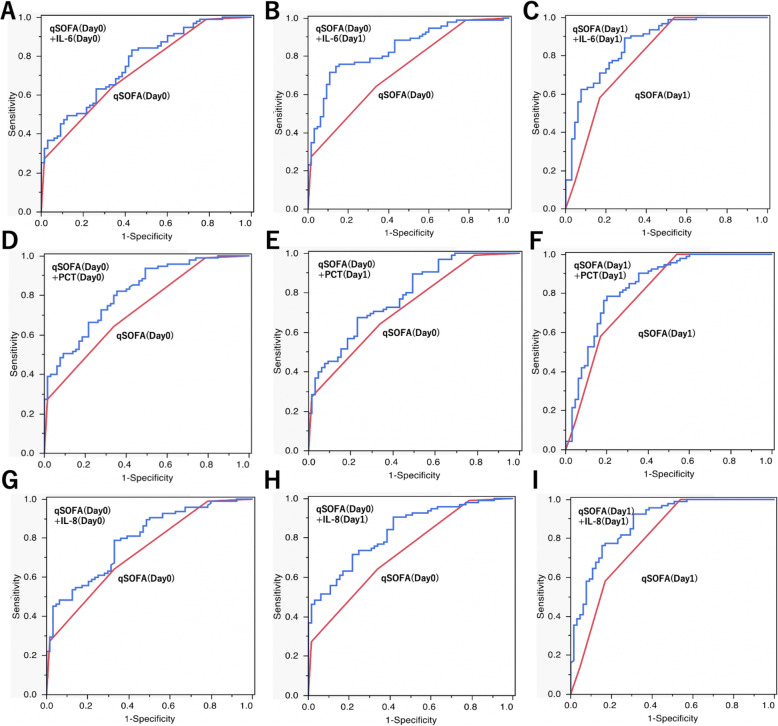
Of 199 patients, 38 were excluded and 161 were included. Patients with MOD on Day 2 had significantly higher qSOFA, SOFA, and Acute Physiology and Chronic Health Evaluation II scores and a trend toward worse prognosis, including mortality. The AUC for qSOFA score (Day 0) that predicted MOD (Day 2) was 0.728 (95% confidence interval [CI]: 0.651-0.794). IL-6 (Day 1) showed the highest AUC among all biomarkers (0.790 [95% CI: 0.711-852]). The combination of qSOFA (Day 0) and IL-6 (Day 1) showed improved prediction accuracy (0.842 [95% CI: 0.771-0.893]). The combination model using qSOFA (Day 1) and IL-6 (Day 1) also showed a higher AUC (0.868 [95% CI: 0.799-0.915]). The combination model of IL-8 and PCT also showed a significant improvement in AUC.
The addition of IL-6, IL-8 and PCT to qSOFA scores improved the accuracy of early MOD prediction.
由于对入侵的生物反应,重症患者在急诊科会出现休克和器官损伤,细胞因子在其发展过程中发挥重要作用。早期预测多器官功能障碍(MOD)很重要,因为这有助于预测患者的预后并选择治疗策略。本研究比较了细胞因子白细胞介素(IL)-6 等生物标志物与快速序贯器官衰竭评估(qSOFA)预测重症患者早期 MOD 的准确性。
这是一项多中心观察性子研究。2016 年至 2018 年,来自五所大学。前瞻性评估了有全身炎症反应综合征表现的成年患者的数据,这些患者就诊于急诊科或入住重症监护病房。在第 0、1 和 2 天评估 qSOFA 评分和每个生物标志物(IL-6、IL-8、IL-10、肿瘤坏死因子-α、C 反应蛋白和降钙素原 [PCT])水平。主要结局是第 2 天的 MOD,分析曲线下面积(AUC)以评估 qSOFA 评分和生物标志物水平。
在 199 名患者中,有 38 名被排除,161 名被纳入。第 2 天发生 MOD 的患者的 qSOFA、SOFA 和急性生理学和慢性健康评估 II 评分显著更高,且预后更差,包括死亡率。qSOFA 评分(第 0 天)预测第 2 天 MOD 的 AUC 为 0.728(95%置信区间[CI]:0.651-0.794)。所有生物标志物中,IL-6(第 1 天)的 AUC 最高(0.790 [95%CI:0.711-852])。qSOFA(第 0 天)和 IL-6(第 1 天)的组合显示出改善的预测准确性(0.842 [95%CI:0.771-0.893])。使用 qSOFA(第 1 天)和 IL-6(第 1 天)的组合模型也显示出更高的 AUC(0.868 [95%CI:0.799-0.915])。IL-8 和 PCT 的组合模型也显示 AUC 显著提高。
将 IL-6、IL-8 和 PCT 添加到 qSOFA 评分中可提高早期 MOD 预测的准确性。