Ramasamy Chidambaram, Mishra Ajay Kumar, John Kevin John, Lal Amos
Department of Internal Medicine, Saint Vincent Hospital, Worcester, MA 01608, United States.
Department of Medicine, Bangalore Baptist Hospital, Bangalore 578954, India.
World J Clin Cases. 2021 Oct 6;9(28):8441-8452. doi: 10.12998/wjcc.v9.i28.8441.
The World Health Organization (WHO) on March 11, 2020, had declared the novel coronavirus disease 2019 (COVID-19) outbreak a global pandemic. The COVID-19 infection continues to be a pandemic and is currently causing overwhelming challenges to healthcare across the nations. Cancer patients represent a unique population vulnerable to COVID-19 infection due to their advanced age, intrinsic frailty, medical comorbidities, immunosuppression, and frequent health care visits for their underlying disease. Robust analysis of COVID-19 infection among cancer patients is crucial to aid in the optimal management of these patients.
To identify contributors of worse outcomes in patients with malignancy and COVID-19 and to describe the role of critical care.
In this review, we summarized the information from seminal articles on the presentation and management of patients with COVID-19 and malignancy that were published before December 10, 2020. We searched the Pub Med and Medline database for "COVID-19" and "Cancer", "Malignancy". Studies published in English, including adults with malignancy and COVID-19 infection, were eligible to be included in this review. Studies on patients that provided details on malignancy, clinical presentation, management, and outcome were included. Various details of malignancy that were included are the site of cancer, histopathological type, stage, chemotherapy, and immunotherapy. Details of COVID-19 infection that were obtained are clinical presentation, the modality of testing, imaging, management, and outcome. Critical care details that were obtained were the type of the organ dysfunction and the requirement of organ support measures, requirement of noninvasive, invasive ventilation, management of vasopressor support, and outcome. Articles that did not have patient details, opinions, letters, and articles not published in English were excluded. All articles were reviewed by 2 independent clinicians. Articles were screened for the above terminologies by independent clinicians.
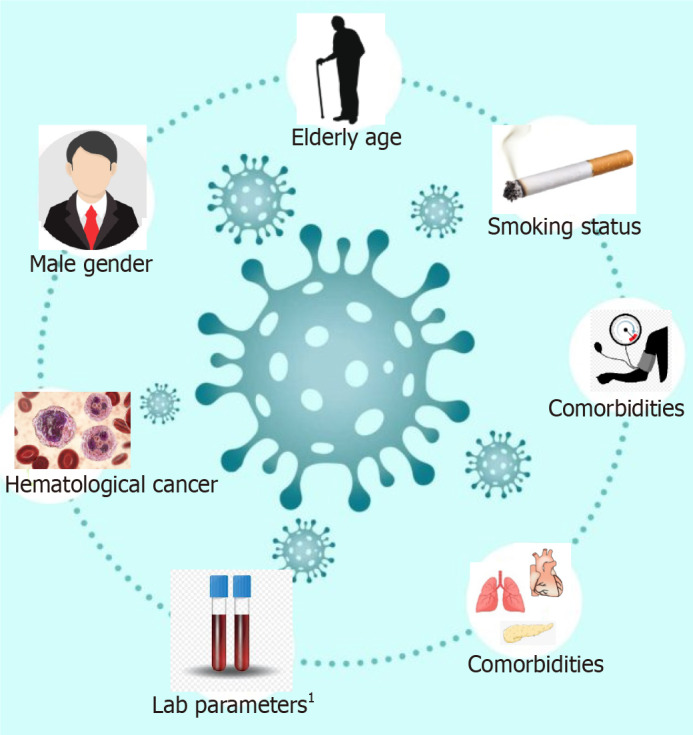
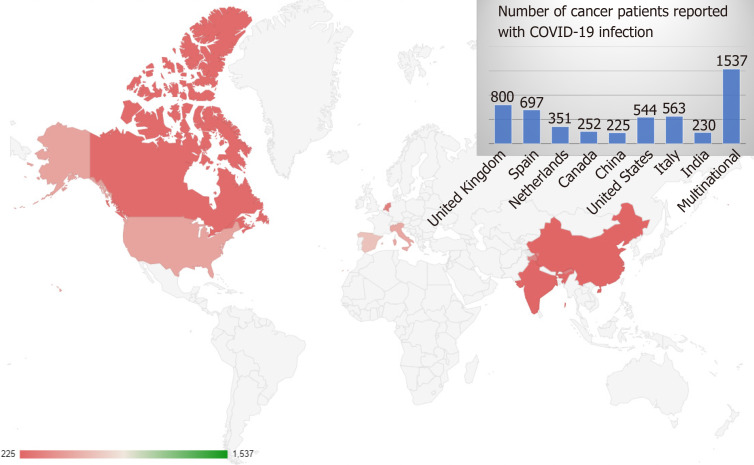
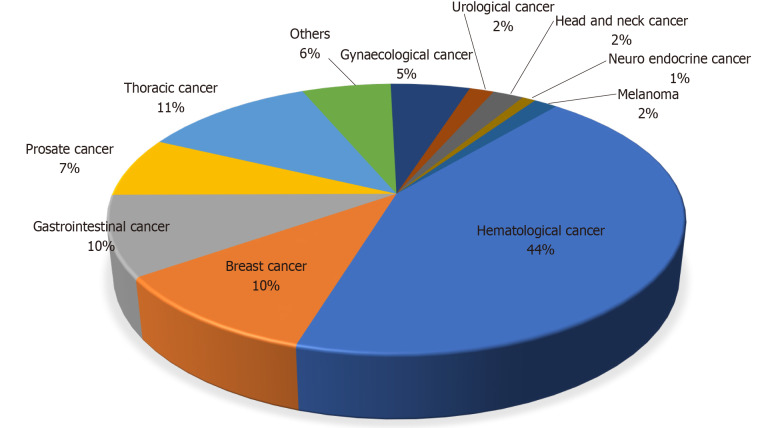
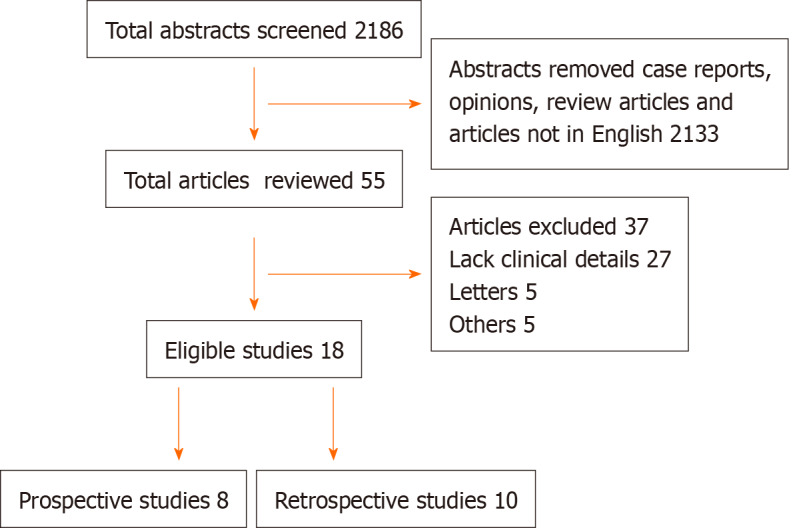
We identified two thousand one hundred eighty-six articles, among which fifty-five were studies that had included patient details pertaining to COVID-19 and cancer (Figure 1). Among these, eighteen studies were eligible and were included in this review as shown in Table 1. A total of 5199 cancer patients were reported. The mean age of patients across all the studies was 64.3 years with male predominance was noted in 12 studies. The clinical presentation and diagnosis of these patients were similar to the general population. Most commonly reported malignancies with COVID-19 infection were hematological in 44% of patients, followed by thoracic malignancy in 11% of patients. The mean number of cancer patients with COVID-19 requiring critical care was 16%. The mean mortality reported was 27.4%. Among the studies that reported the presence of organ dysfunction, respiratory failure was reported in 52% of patients, of which 11.7% required mechanical ventilation. 72% of COVID-19 cancer patients required hospitalization across all the studies. The factors which are associated with the worse outcome from COVID-19 infections among the cancer patients were male gender, age ≥ 65 years, presence of higher comorbidity burden based on Charlson comorbidity index and cumulative illness reporting scale > 6, and smoking history.
The majority of the cancer patients required intensive care due to respiratory failure and the need for mechanical ventilation. Appropriate contingency planning for these patients in terms of goals of care and judicious resource allocation in the resource-poor regions is the key. The factors associated with worse outcomes from COVID-19 infections were independent of oncological features such as tumor stage, disease status, or current provision of active anticancer therapy and it could be continued with caution.
2020年3月11日,世界卫生组织(WHO)宣布2019年新型冠状病毒病(COVID-19)疫情为全球大流行。COVID-19感染仍是一场大流行疾病,目前给世界各国的医疗保健带来了巨大挑战。癌症患者因其年龄较大、体质虚弱、合并症、免疫抑制以及因基础疾病而频繁就医等因素,成为易受COVID-19感染的特殊人群。对癌症患者中的COVID-19感染进行有力分析,对于帮助优化这些患者的管理至关重要。
确定恶性肿瘤合并COVID-19患者预后较差的影响因素,并描述重症监护的作用。
在本综述中,我们总结了2020年12月10日前发表的关于COVID-19合并恶性肿瘤患者的临床表现和管理的重要文章中的信息。我们在PubMed和Medline数据库中搜索了“COVID-19”以及“癌症”“恶性肿瘤”。纳入本综述的研究需为英文发表,包括患有恶性肿瘤并感染COVID-19的成年人。纳入提供了恶性肿瘤、临床表现、管理和预后详细信息的患者研究。纳入的恶性肿瘤的各种详细信息包括癌症部位、组织病理学类型、分期、化疗和免疫治疗。获取的COVID-19感染详细信息包括临床表现、检测方式、影像学检查、管理和预后。获取的重症监护详细信息包括器官功能障碍类型和器官支持措施的需求、无创和有创通气的需求、血管活性药物支持的管理以及预后。未包含患者详细信息、观点、信函以及非英文发表的文章被排除。所有文章均由2名独立的临床医生进行评审。独立临床医生根据上述术语对文章进行筛选。
我们共检索到2186篇文章,其中55篇为包含COVID-19和癌症患者详细信息的研究(图1)。其中,18项研究符合要求并纳入本综述,如表1所示。共报告了5199例癌症患者。所有研究中患者的平均年龄为64.3岁,12项研究中男性占多数。这些患者的临床表现和诊断与一般人群相似。COVID-19感染最常报告的恶性肿瘤类型中,血液系统恶性肿瘤占44%的患者,其次是胸部恶性肿瘤占11%的患者。需要重症监护的COVID-19癌症患者的平均比例为16%。报告的平均死亡率为27.4%。在报告存在器官功能障碍的研究中,52%的患者出现呼吸衰竭,其中11.7%的患者需要机械通气。所有研究中72%的COVID-19癌症患者需要住院治疗。癌症患者中与COVID-19感染预后较差相关的因素包括男性、年龄≥65岁、基于Charlson合并症指数的合并症负担较高以及累积疾病报告量表>6分,以及吸烟史。
大多数癌症患者因呼吸衰竭和需要机械通气而需要重症监护。在资源匮乏地区,针对这些患者在治疗目标和合理资源分配方面制定适当的应急计划是关键。与COVID-19感染预后较差相关的因素独立于肿瘤特征,如肿瘤分期、疾病状态或当前是否进行积极的抗癌治疗,可谨慎继续进行。