Rocky Vista University College of Osteopathic Medicine, Parker, CO, USA.
Rocky Vista University College of Osteopathic Medicine, Parker, CO, USA.
Am J Emerg Med. 2022 Apr;54:326.e1-326.e4. doi: 10.1016/j.ajem.2021.10.023. Epub 2021 Oct 25.
COVID-19 has profound direct health consequences, however secondary effects were much broader as rates of hospital visits steeply declined for non-COVID-19 concerns, including myocardial infarction (MI) and stroke, with patients choosing to wait longer before symptoms convince them to seek medical attention. Thus, patients where ischemia leads to tissue loss should be a major concern.
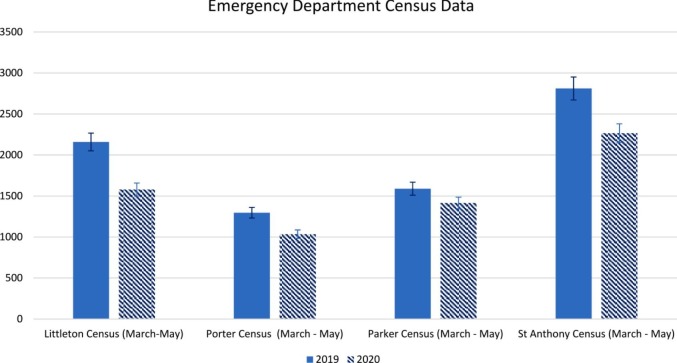
The months of March to June 2019 and 2020 were compared to each other at 4 Denver area hospitals. Reduction in overall ED visits and an increase in patient refusal for emergency transport were clear in the data collected. During this period in 2019, 49 MI and 90 stroke patients were admitted. In 2020 this was 40 and 90 respectively. All were matched for age and gender. For MI patients ejection fraction and door to EKG and intervention times were measured. For stroke patients last known well time, time to evaluation, and modified Rankin scores were measured.
254 (8.12%) patients refused emergency services transportation before the pandemic compared to 479 (18.35%) during the pandemic (p-value <0.001, chi square test). In the MI cohort, no significant difference was detected in measured ejection fraction (48% vs 49% p-value = 0.682). Additionally, no significant difference was detected between door to EKG time or door to MI intervention time. During the pandemic 8 (22%) expired with an MI prior to discharge, compared to 2 (4%) before the pandemic. The stroke cohort Door to Evaluation Time, Time since last well known, and modified Rankin scores were all found to have insignificant differences.
ED volume was significantly lower during the early stages of the pandemic. During this time however only death from cardiac events increased, in spite of similar ejection fractions at discharge. The cause of this remains unclear as ejection fraction similarities make it less attributable to loss of tissue than to other factors. Patient behavior significantly changed during the pandemic, making this a likely source of the increase in mortality seen.
COVID-19 对健康有深远的直接影响,但次生影响更为广泛,因为非 COVID-19 疾病的住院率急剧下降,包括心肌梗死(MI)和中风,患者选择在症状出现更长时间后才去就医。因此,缺血导致组织损失的患者应引起重视。
在丹佛地区的 4 家医院比较了 2019 年 3 月至 6 月和 2020 年同期的数据。收集的数据清楚地显示,急诊就诊总量减少,以及患者拒绝紧急转运的情况明显增加。在 2019 年同期,有 49 例 MI 和 90 例中风患者入院。而在 2020 年,这一数字分别为 40 例和 90 例。所有患者均按年龄和性别匹配。对于 MI 患者,测量射血分数、从到心电图(EKG)和介入时间。对于中风患者,测量最后一次正常时间、评估时间和改良 Rankin 评分。
与大流行前相比,254 例(8.12%)患者在大流行期间拒绝接受紧急服务转运,而 479 例(18.35%)患者在大流行期间拒绝接受紧急服务转运(p 值<0.001,卡方检验)。在 MI 队列中,测量的射血分数(48%比 49%,p 值=0.682)没有显著差异。此外,EKG 时间或 MI 介入时间之间没有显著差异。在大流行期间,有 8 例(22%)MI 患者在出院前死亡,而大流行前有 2 例(4%)。在中风队列中,评估时间、最后一次正常状态到发病时间和改良 Rankin 评分均无显著差异。
在大流行早期,急诊就诊量显著减少。然而,在此期间,只有心脏病事件的死亡率增加,尽管出院时的射血分数相似。这种情况的原因尚不清楚,因为射血分数相似性使其不太归因于组织损失,而更归因于其他因素。患者行为在大流行期间发生了显著变化,这可能是观察到的死亡率增加的原因。