Bruce Julie, Mazuquin Bruno, Canaway Alastair, Hossain Anower, Williamson Esther, Mistry Pankaj, Lall Ranjit, Petrou Stavros, Lamb Sarah E, Rees Sophie, Padfield Emma, Vidya Raghavan, Thompson Alastair M
Warwick Clinical Trials Unit, Division of Health Sciences, University of Warwick, Coventry, UK
Faculty of Health, Psychology and Social Care, Manchester Metropolitan University, Manchester, UK.
BMJ. 2021 Nov 10;375:e066542. doi: 10.1136/bmj-2021-066542.
To evaluate whether a structured exercise programme improved functional and health related quality of life outcomes compared with usual care for women at high risk of upper limb disability after breast cancer surgery.
Multicentre, pragmatic, superiority, randomised controlled trial with economic evaluation.
17 UK National Health Service cancer centres.
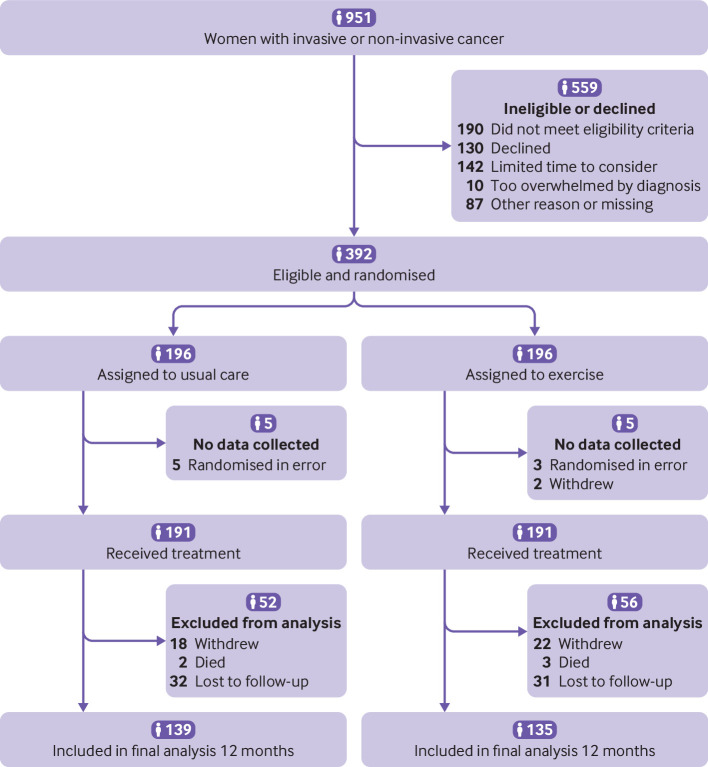
392 women undergoing breast cancer surgery, at risk of postoperative upper limb morbidity, randomised (1:1) to usual care with structured exercise (n=196) or usual care alone (n=196).
Usual care (information leaflets) only or usual care plus a physiotherapy led exercise programme, incorporating stretching, strengthening, physical activity, and behavioural change techniques to support adherence to exercise, introduced at 7-10 days postoperatively, with two further appointments at one and three months.
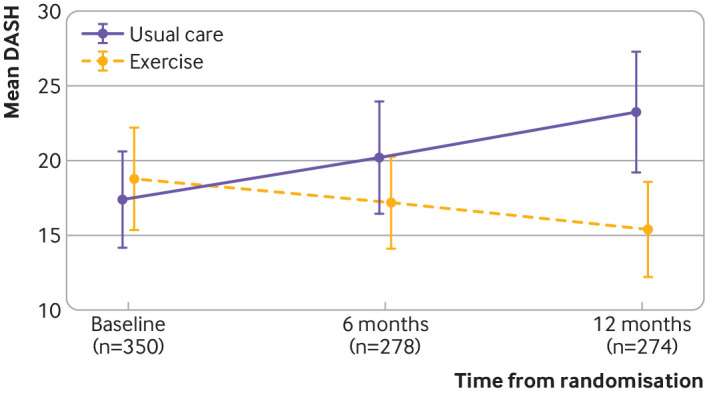
Disability of Arm, Hand and Shoulder (DASH) questionnaire at 12 months, analysed by intention to treat. Secondary outcomes included DASH subscales, pain, complications, health related quality of life, and resource use, from a health and personal social services perspective.
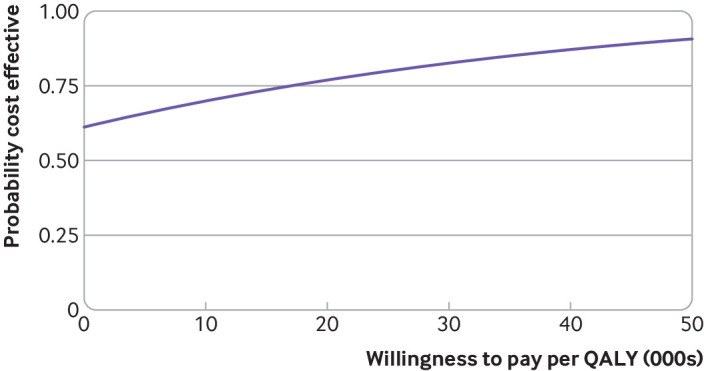
Between 26 January 2016 and 31 July 2017, 951 patients were screened and 392 (mean age 58.1 years) were randomly allocated, with 382 (97%) eligible for intention to treat analysis. 181 (95%) of 191 participants allocated to exercise attended at least one appointment. Upper limb function improved after exercise compared with usual care (mean DASH 16.3 (SD 17.6) for exercise (n=132); 23.7 (22.9) usual care (n=138); adjusted mean difference 7.81, 95% confidence interval 3.17 to 12.44; P=0.001). Secondary outcomes favoured exercise over usual care, with lower pain intensity at 12 months (adjusted mean difference on numerical rating scale -0.68, -1.23 to -0.12; P=0.02) and fewer arm disability symptoms at 12 months (adjusted mean difference on Functional Assessment of Cancer Therapy-Breast+4 (FACT-B+4) -2.02, -3.11 to -0.93; P=0.001). No increase in complications, lymphoedema, or adverse events was noted in participants allocated to exercise. Exercise accrued lower costs per patient (on average -£387 (€457; $533) (95% confidence interval -£2491 to £1718; 2015 pricing) and was cost effective compared with usual care.
The PROSPER exercise programme was clinically effective and cost effective and reduced upper limb disability one year after breast cancer treatment in patients at risk of treatment related postoperative complications.
ISRCTN Registry ISRCTN35358984.
评估与乳腺癌手术后有上肢残疾高风险女性的常规护理相比,结构化运动方案是否能改善功能及与健康相关的生活质量结果。
多中心、实用、优效性、随机对照试验并进行经济评估。
17家英国国民保健服务癌症中心。
392例接受乳腺癌手术且有术后上肢发病风险的女性,随机(1:1)分为接受常规护理加结构化运动(n = 196)或仅接受常规护理(n = 196)。
仅常规护理(信息手册)或常规护理加由物理治疗师主导的运动方案,包括拉伸、强化训练、身体活动及行为改变技巧以支持坚持运动,术后7 - 10天开始,术后1个月和3个月还有两次预约。
术后12个月时的手臂、手部和肩部残疾(DASH)问卷,采用意向性分析。次要结局包括从健康和个人社会服务角度的DASH分量表、疼痛、并发症、与健康相关的生活质量及资源使用情况。
2016年1月26日至2017年7月31日期间,筛查了951例患者,392例(平均年龄58.1岁)被随机分配,382例(97%)符合意向性分析条件。分配到运动组的191例参与者中有181例(95%)至少参加了一次预约。与常规护理相比,运动后上肢功能得到改善(运动组平均DASH为16.3(标准差17.6)(n = 132);常规护理组为23.7(22.9)(n = 138);调整后平均差异为7.81,95%置信区间为3.17至12.44;P = 0.001)。次要结局显示运动优于常规护理,术后12个月时疼痛强度更低(数字评定量表调整后平均差异为 - 0.68, - 1.23至 - 0.12;P = 0.02),术后12个月时手臂残疾症状更少(癌症治疗功能评估 - 乳腺 + 4(FACT - B + 4)调整后平均差异为 - 2.02, - 3.11至 - 0.93;P = 0.001)。分配到运动组的参与者未发现并发症、淋巴水肿或不良事件增加。运动使每位患者的成本更低(平均 - 387英镑(457欧元;533美元)(95%置信区间为 - 2491英镑至1718英镑;2015年定价),与常规护理相比具有成本效益。
PROSPER运动方案在临床上有效且具有成本效益,可降低乳腺癌治疗后有治疗相关术后并发症风险患者一年后的上肢残疾程度。
国际标准随机对照试验编号ISRCTN35358984。