Varsha R, Desai Sameer N, Mudakanagoudar Mahantesh S, Annigeri Venkatesh M
Department of Anaesthesiology, SDM College of Medical Sciences and Hospital, Dharawd, Karnataka, India.
Department of Paediatric Surgery, SDM College of Medical Sciences and Hospital, Dharawd, Karnataka, India.
J Anaesthesiol Clin Pharmacol. 2021 Jul-Sep;37(3):389-394. doi: 10.4103/joacp.JOACP_175_19. Epub 2021 Oct 12.
Caudal epidural and ultrasound-guided ilioinguinal, iliohypogastric nerve (IL/IH) blocks are commonly used regional anesthesia techniques for postoperative analgesia in pediatric inguinal surgeries. Dexmedetomidine as an adjuvant has been proven to prolong the duration of both neuraxial and peripheral nerve blocks. We compared the duration of analgesia provided by local anesthetic (LA) and dexmedetomidine for caudal and IL/IH block for pediatric inguinal surgeries.
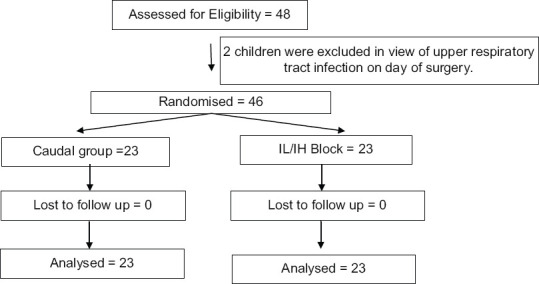
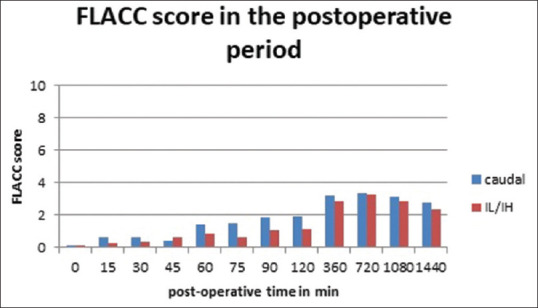
Forty-six children undergoing inguinal hernia repair were selected for this randomized double-blind study. After general anesthesia, children received either 0.75 mL.kg of 0.25% bupivacaine with 1 mcg.kg of dexmedetomidine in caudal epidural or 0.25 mL.kg of 0.25% bupivacaine with 1 mcg.kg of dexmedetomidine in IL/IH block. The pain was assessed up to 24 h postoperatively using face, legs, activity, cry, consolability (FLACC) score. For FLACC ≥4, rescue analgesia was provided using 1 μg/kg of intravenous fentanyl, up to 2 h postoperatively and 10 mg/kg of oral ibuprofen between 2 and 24 postoperative hours. The time for first rescue analgesia was taken as the duration of analgesia.
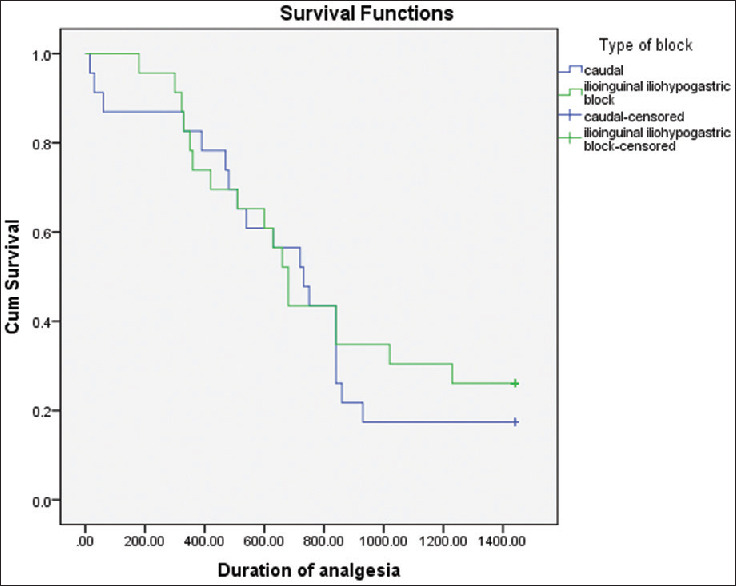
There were no significant differences in the pain scores or analgesic utilization between the groups. The duration of analgesia of caudal and IL/IH blocks was similar (720.3 ± 430.1 min and 808.4 ± 453.1 min, respectively). The time taken for the performance of block was significantly higher for caudal compared to IL/IH (547 ± 93 vs. 317 ± 179 s; < 0.001).
Both caudal epidural and USG-IL/IH block with dexmedetomidine as additive provide the comparable duration of postoperative analgesia with no significant side effects.
骶管硬膜外阻滞和超声引导下髂腹股沟、髂腹下神经(IL/IH)阻滞是小儿腹股沟手术术后镇痛常用的区域麻醉技术。右美托咪定作为辅助用药已被证明可延长椎管内和周围神经阻滞的时间。我们比较了局部麻醉药(LA)联合右美托咪定用于小儿腹股沟手术骶管阻滞和IL/IH阻滞的镇痛持续时间。
本随机双盲研究选取了46例行腹股沟疝修补术的儿童。全身麻醉后,儿童在骶管硬膜外阻滞中接受0.75 mL/kg的0.25%布比卡因加1 mcg/kg右美托咪定,或在IL/IH阻滞中接受0.25 mL/kg的0.25%布比卡因加1 mcg/kg右美托咪定。术后24小时内使用面部、腿部、活动、哭闹、安慰度(FLACC)评分评估疼痛。对于FLACC≥4的情况,术后2小时内使用1 μg/kg静脉注射芬太尼进行补救镇痛,术后2至24小时使用10 mg/kg口服布洛芬进行补救镇痛。首次补救镇痛的时间作为镇痛持续时间。
两组之间的疼痛评分或镇痛药物使用情况无显著差异。骶管阻滞和IL/IH阻滞的镇痛持续时间相似(分别为720.3±430.1分钟和808.4±453.1分钟)。与IL/IH阻滞相比,骶管阻滞的操作时间明显更长(547±93秒对317±179秒;P<0.001)。
骶管硬膜外阻滞和超声引导下IL/IH阻滞联合右美托咪定作为添加剂提供了相当的术后镇痛持续时间,且无明显副作用。