Song Zijia, Liu Kun, Li You, Shi Yiqing, Jiang Yimei, Wang Changgang, Chen Xianze, Zhang Tao, Ji Xiaopin, Zhao Ren
Department of General Surgery, Ruijin Hospital, Shanghai Jiaotong University School of Medicine, Shanghai, China.
Front Oncol. 2021 Oct 25;11:762147. doi: 10.3389/fonc.2021.762147. eCollection 2021.
To date, well-designed randomized controlled trials examining the safety, efficacy, and long-term outcomes of single-incision laparoscopic surgery (SILS) for colorectal cancer are scarce. The aim of the current study was to compare short-term outcomes of SILS for colorectal cancer with conventional laparoscopic surgery (CLS).
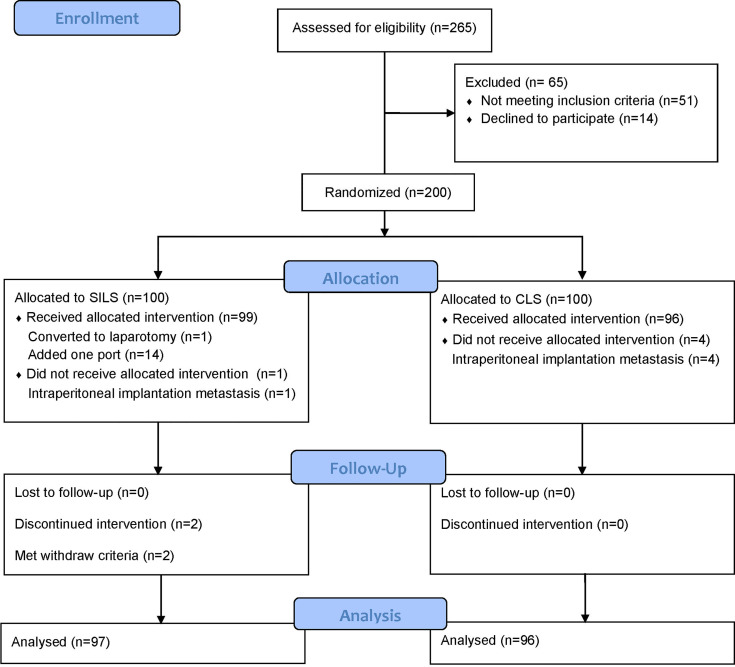
Between June 28, 2017, and June 29, 2019, a single-center, open-label, non-inferiority, randomized clinical trial was conducted at the Department of General Surgery, Ruijin Hospital (North), Shanghai Jiaotong University School of Medicine in Shanghai, China. In total, 200 patients diagnosed or suspected of colorectal cancer (cTNM) were randomly assigned to either the SILS or CLS group in a 1:1 ratio. The primary outcome was early morbidity rate. Secondary outcomes included intraoperative outcomes, pain intensity, postoperative recovery, pathologic outcomes, and long-term outcomes.
In total, 193 participants (SILS, 97; CLS, 96) were analyzed in the modified intention-to-treat (MITT) population. Among them, 48 underwent right hemicolectomy (SILS = 23, 23.7% and MLS = 25, 26%), 15 underwent left hemicolectomy (SILS = 6, 6.2% and MLS = 9, 9.4%), 1 underwent transverse colectomy (MLS = 1, 1%), 57 underwent sigmoidectomy (SILS = 32, 33% and MLS = 25, 26%), and 72 underwent anterior resection (SILS = 36, 37.1% and MLS = 36, 37.5%). No significant differences were observed in the baseline characteristics. The intraoperative complication was comparable between the two groups [5 (5.2%) vs. 4 (4.2%); difference, 1%; 95% CI, -5.8% to 7.8%; > 0.999) and so was postoperative complication rates [10 (10.3%) vs. 14 (14.6%); difference, -4.3%; 95% CI, -13.9% to 5.3%; = 0.392]. The SILS group showed shorter incision length [median (IQR), 4 (3.5-5) vs. 6.6 (6-7.5), < 0.001] and lower VAS scores on the first [median (IQR), 4 (3-5) vs. 4 (4-5), = 0.002] and the second day [median (IQR), 2 (1.5-3) vs. 3 (2-4), < 0.001] after surgery. No statistically significant difference was found in other measured outcomes.
Compared with CLS, SILS performed by experienced surgeons for selected colorectal cancer patients is non-inferior with good short-term safety and has the advantage of reducing postoperative pain.
ClinicalTrials.gov, identifier NCT03151733.
迄今为止,针对单孔腹腔镜手术(SILS)治疗结直肠癌的安全性、有效性及长期预后进行的设计良好的随机对照试验较为匮乏。本研究旨在比较SILS与传统腹腔镜手术(CLS)治疗结直肠癌的短期预后。
2017年6月28日至2019年6月29日,在中国上海交通大学医学院附属瑞金医院(北院)普外科开展了一项单中心、开放标签、非劣效性随机临床试验。总共200例诊断或疑似结直肠癌(cTNM)患者按1:1比例随机分配至SILS组或CLS组。主要结局为早期发病率。次要结局包括术中结局、疼痛强度、术后恢复、病理结局及长期结局。
在改良意向性分析(MITT)人群中,共分析了193例参与者(SILS组97例,CLS组96例)。其中,48例行右半结肠切除术(SILS组23例,占23.7%;CLS组25例,占26%),15例行左半结肠切除术(SILS组6例,占6.2%;CLS组9例,占9.4%),1例行横结肠切除术(CLS组1例,占1%),57例行乙状结肠切除术(SILS组32例,占33%;CLS组25例,占26%),72例行前切除术(SILS组36例,占37.1%;CLS组36例,占37.5%)。两组基线特征未见显著差异。两组术中并发症相当[5例(5.2%)对4例(4.2%);差异1%;95%CI,-5.8%至7.8%;P>0.999],术后并发症发生率也相当[10例(10.3%)对14例(14.6%);差异-4.3%;95%CI,-13.9%至5.3%;P=0.392]。SILS组切口长度较短[中位数(四分位间距),4(3.5 - 5)对6.6(6 - 7.5),P<0.001],术后第1天[中位数(四分位间距),4(3 - 5)对4(4 - 5),P=0.002]和第2天[中位数(四分位间距),2(1.5 - 3)对3(2 - 4),P<0.001]视觉模拟评分(VAS)较低。其他测量结局未见统计学显著差异。
对于经选择的结直肠癌患者,由经验丰富的外科医生实施的SILS与CLS相比非劣效,具有良好的短期安全性且有减轻术后疼痛的优势。
ClinicalTrials.gov,标识符NCT03151733 。